gonefishing
Forum Deputy Chief
- 1,374
- 412
- 83
Now its $100 every 30 minutes.???
I've definitely never heard of this and can't find anything on LA county's website.
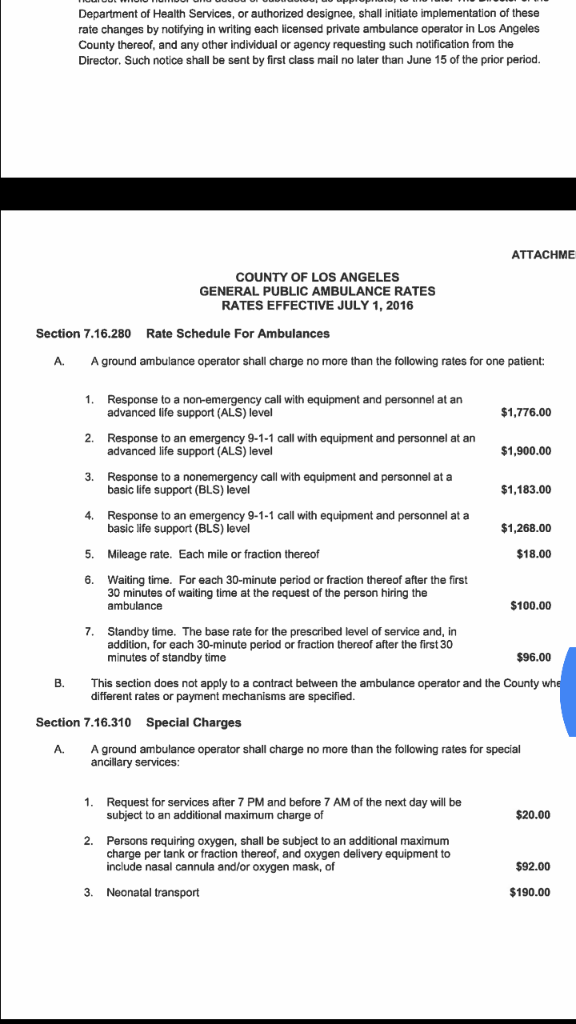
Sent from my SM-G920P using Tapatalk
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Now its $100 every 30 minutes.???
I've definitely never heard of this and can't find anything on LA county's website.
Now its $100 every 30 minutes.
Sent from my SM-G920P using Tapatalk
Yea. Alot of paper tickets use to have a check box. Or that's why most places ask that after 20 minutes you give an update so they can start the clock at the 30 mark to ensure they bill properly. Clock doesn't stop until on your electronic pcr you mark tx of care. On paper you had to write down that time. This all goes to the pt or the pt's insurance.But... I don't think said person has a choice whether to "request" us to wait. It's not like we can just dump the patient in the hallway? But if so, I didn't realize this was a thing. Interesting, thanks.
Yea. Alot of paper tickets use to have a check box. Or that's why most places ask that after 20 minutes you give an update so they can start the clock at the 30 mark to ensure they bill properly. Clock doesn't stop until on your electronic pcr you mark tx of care. On paper you had to write down that time. This all goes to the pt or the pt's insurance.
Sent from my SM-G920P using Tapatalk
Not at all. That's all cash. Not as much as a run but still a pretty good amount of cash for doing nothing. It's more than paying for you and your partners wage per hour.Ahh, that makes sense. Yeah, we get a status request after 20 minutes and mark tx of care time on our epcr. Thanks for the info. I thought our company just eats the cost of us having to the hold wall.
I think more or less what he was pointing out was that your fortunate that your system has more beds and more staff to fit your population needs where as here in California, the population has skyrocketed in certain areas out doing the supply. Almost like economics 101 supply and demand. You have say 2 hospitals both with 10 er beds equaling out to 20. The ppolulation is 8, it grows to 18 in a short period of time. The hospitals can still manage. The population grows to 60 later that year, you still have 20 beds for that population of 60 with enough nursing staff at minimum. Population doubles, you now have no where near enough staff, not enough beds, the supply line (ambulances) clog up and their for the production line like in a factory is held up. That's the real issue. The population is growing faster than what the resources in place can keep up with or change with.Nowhere did i say im a better paramedic, nor that my organization is superior; but I can unequivocally state my system runs better.
If you think expecting to clear a call in less than an hour from arrival at the back doors makes me spoiled, then I simply don't know what to say to you. I think expecting a crew to hold the wall for hours on end due to a broken healthcare system is absolutely unreasonable, but we're all walking our own path, so you do you.
And yes, if I had no choice but to work in such a system or do something else, I would seek out career alternatives.
Waving the BS flag as hard as I can!!!!!I think more or less what he was pointing out was that your fortunate that your system has more beds and more staff to fit your population needs where as here in California, the population has skyrocketed in certain areas out doing the supply. Almost like economics 101 supply and demand. You have say 2 hospitals both with 10 er beds equaling out to 20. The ppolulation is 8, it grows to 18 in a short period of time. The hospitals can still manage. The population grows to 60 later that year, you still have 20 beds for that population of 60 with enough nursing staff at minimum. Population doubles, you now have no where near enough staff, not enough beds, the supply line (ambulances) clog up and their for the production line like in a factory is held up. That's the real issue. The population is growing faster than what the resources in place can keep up with or change with.
IIRC, wait time gets billed directly to the patient, as the insurance company won't pay it.Now its $100 every 30 minutes.
Yes true as state as a whole population is not the highest BUT certain once small town areas have seen population booms in a small short period of time and or more people are using the ED as their physician. I agree hospitals need to higher more staff, stop using ems as free labor. Their is an exception to the wait time fee being passed to the patient. Such insurance companys as Kaiser Permanente do NOT pass the cost to the patient. I worked with a company that held that contract and kp gladly paid the fee. By the way, we also have a nursing shortage.Waving the BS flag as hard as I can!!!!!
1) California is not the densest state in the union. In fact, the top 4 densest counties in the US aren't in California (they are all in NYC). Los Angeles might be the largest county by population, but that's spread over 4,000 square miles. When you go into densest cities in the US, Los Angeles isn't even in the top 10 (but San Francisco is). And you don't hear about people in NY, NJ, Massachusetts, Pennsylvania, DC or Virginia ever holding the wall for hours (that's the top 10 btw). So the argument that California's population has skyrocketed is crap, because populations in every metro area has skyrocketed, but only California has type of system and accepts this issues as acceptable.
2) I don't doubt that the hospitals need more beds, more nurses, and more staff. So what's stopping them? There is obviously a need. If the hospitals haven't keep up with demand, than they need new administration to actually move forward and expand. Random surges happen to everyone, but if you are constantly in a surge mode, than that's not a surge, that's normal operations. If EMS kept the same number of ambulances that they had in the 90s, with the growing call volume, would that be considered acceptable? so why is it acceptable that the hospitals haven't grown? If other hospitals have been able to grow, maybe California hospitals needs to learn how to budget and do long term planning? there are poor areas everywhere, so the argument of "well we have no money" is crap, because they still find ways to fund expansions (they are called capital investments).
3) this whole system is a hospital issue, and EMS shouldn't be providing free labor to the hospital. I know of one agency that actually sent the hospital a bill for all the time holding the wall. Administration didn't like it, and did complain, but they provided a service for the hospital, and they shouldn't operate free of charge. I'm surprised more agencies haven't done that.
4) I agree with @hometownmedic5 , I wouldn't work in a system where I had to hold a wall, regardless of if I have a BS patient or not. In fact, I would probably start harassing the nurses after the 30 minute mark until they both threw me out of the ER and called me boss and complained, at which point his response should be "well, if you gave him a bed, he would leave you alone, and he could get back to doing the job I'm paying him to do, instead of him doing the job that you are paid to do."
IIRC, wait time gets billed directly to the patient, as the insurance company won't pay it.
and that was exactly what I was wondering, maybe if enough patient's were billed, and then complained about the bills to the hospitals (who are the cause of them receiving this bills), they would improve their system. I don't like billing the patient for a hospital issue, but I like having the company eat the cost even less, as it contributes to why EMS gets paid so poorly, because they are stuck in the ERs not making money for their companies and costing them the hourly rate.
Maybe more people should start doing that and they will get the point.Our county actually allows that now. After 30 minutes on bed delay with a BLS patient we will sit them on a chair and have them hold their paperwork and tell that staff “hey guys, he is sitting here. Bye”
But not every patient can sit in a chair lol what about your bed confined geriatric with a low hemoglobin that was sent to the ED?Maybe more people should start doing that and they will get the point.
I have a big issue with wait times being billed to the patient. They would be better off if you found them a chair.
Sent from my SAMSUNG-SM-G920A using Tapatalk
What’s worse is that by the county we are given that right but our company policies do not allow us to do it.Maybe more people should start doing that and they will get the point.
I have a big issue with wait times being billed to the patient. They would be better off if you found them a chair.
Sent from my SAMSUNG-SM-G920A using Tapatalk
Lay them in 3 chairs?But not every patient can sit in a chair lol what about your bed confined geriatric with a low hemoglobin that was sent to the ED?
Sent from my SM-G920P using Tapatalk
this happens all over, it's not limited to California. And I didn't mention total state numbers (with California would lead, because it is the largest geographic state in the US), that was only county and city. That's why I referenced population density, because size is all relative, but density is constant (how many people do you have in a square mile, etc). And the two densest cities in the US are Gutenberg, Union City, West New York, and Bayonne, all in Hudson County NJ (and they don't have nearly the issues with hospital wall time that you are describing). New York City isn't even in the top 5Yes true as state as a whole population is not the highest BUT certain once small town areas have seen population booms in a small short period of time and or more people are using the ED as their physician.
By the way, there is a nursing shortage everywhere. Actually, that's not true; many hospitals don't want to hire new grads, or pay them well, or give them the support to do their jobs, so they don't want to work for ****ty places (nationwide, not just California). Maybe if they staffed more nurses per shift and didn't run them into the ground they wouldn't have their supposed "nursing shortage" (which was made up by the nursing unions and nursing schools, not by the general public, unless they are taking the word from those two biased groups).By the way, we also have a nursing shortage.
I agree; it should be billed to the entity causing the delay, in this case, the hospital. They are causing the costs to be incurred by the ambulance service, so unless they are forced to pay for it, they are in no position to even try to fix this obviously broken systemI have a big issue with wait times being billed to the patient. They would be better off if you found them a chair.
Your right: the hospital should get them a bed.. you can put them in triage if they need to be (if they are considered low priority), but having the ambulance babysit them isn't helping anyone except for the hospital in not doing their job.But not every patient can sit in a chair lol what about your bed confined geriatric with a low hemoglobin that was sent to the ED?
, the population has skyrocketed in certain areas out doing the supply. Almost like economics 101 supply and demand.
only California has type of system and accepts this issues as acceptable.
By the way, we also have a nursing shortage.
Your hospitals dont have a triage area you can put patients on a bed?
Our 30 room ER has a triage area which has 20 beds and 10 recliners, 2 nurses and 2 techs. EMS gives report to triage and puts them on a bed and hospital sorts it our from there. Even on busy busy days its no more than 20 minutes waiting for report.
By the way, we also have a nursing shortage.
Actually guys, there really isn't a nursing shortage. This is actually cyclical and right now we're on the downslope into a "shortage" but we won't see it for probably another 5 years or so. Why do I say this? Nurses age. If you want to know where any nursing shortage really is if it's anywhere, it's in the supply of experienced nurses. The cost of travelers may actually be less than training/orienting a new grad (and there's lots of new grads) over the course of a year.By the way, there is a nursing shortage everywhere. Actually, that's not true; many hospitals don't want to hire new grads, or pay them well, or give them the support to do their jobs, so they don't want to work for ****ty places (nationwide, not just California).