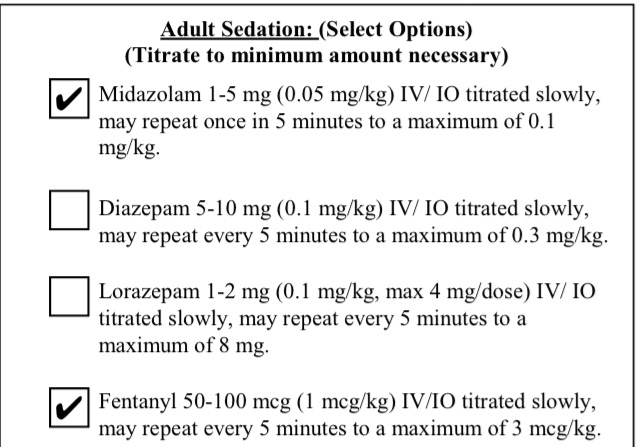
Is anyone allowed to do concurrent pain and sedation for cardioversion or pacing? I've always wondered why we use anxiolytics rather than analgesics since it's a painful procedure. Also, expanding on Nova's thought about getting a little more wiggle room for sedation, wouldn't it be just as if not more effective to use a smaller dose of midazolam concurrently with fentanyl rather than just straight midazolam? Not only is fentanyl very hemodynamically "stable", the smaller dose of midaz is going to to have less vasoactive actions than a big slug of it. The combo can render the same if not better results.
We can do concurrent pain and sedation for pain associated with a large muscle mass such as a femur fracture or back spasms on standing orders, only can use sedation for cardioversion and pacing without OLMD.
As far as the question about fluids, it's been answered well already. Not necessarily going to be a bad thing but if someone is symptomatic enough to warrant cardioversion as the first line treatment why go doinking around getting a line and spiking a bag? It always makes me wonder when people say "while I setup for cardioversion". It takes all of 30 seconds to place pads, select your energy setting and sync the monitor.
Do you know what departments are using a benzo/fent combination for sedation, or for pain management with a Fx? I'd like to present this to EMS admin and the OMD if other departments can