DragonClaw
Emergency Medical Texan
- 2,116
- 363
- 83
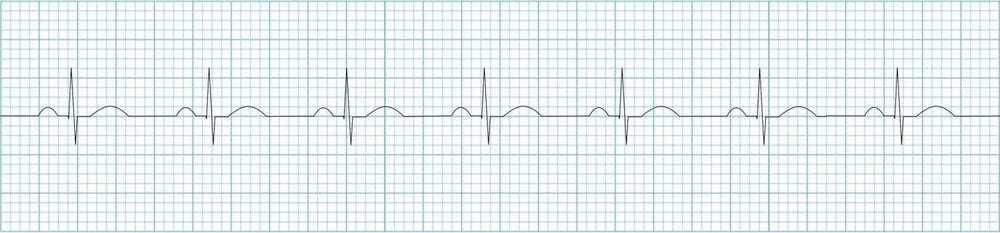
I don't really know how they're saying it's different. Or what to call them to distinguish the two. Is tracing the difference?
Also, I thought cardiac monitoring was a ALS procedure and EMTB wouldn't be doing this? I guess it depends on the medical director though?


Also, I thought cardiac monitoring was a ALS procedure and EMTB wouldn't be doing this? I guess it depends on the medical director though?