ThadeusJ
Forum Lieutenant
- 240
- 69
- 28
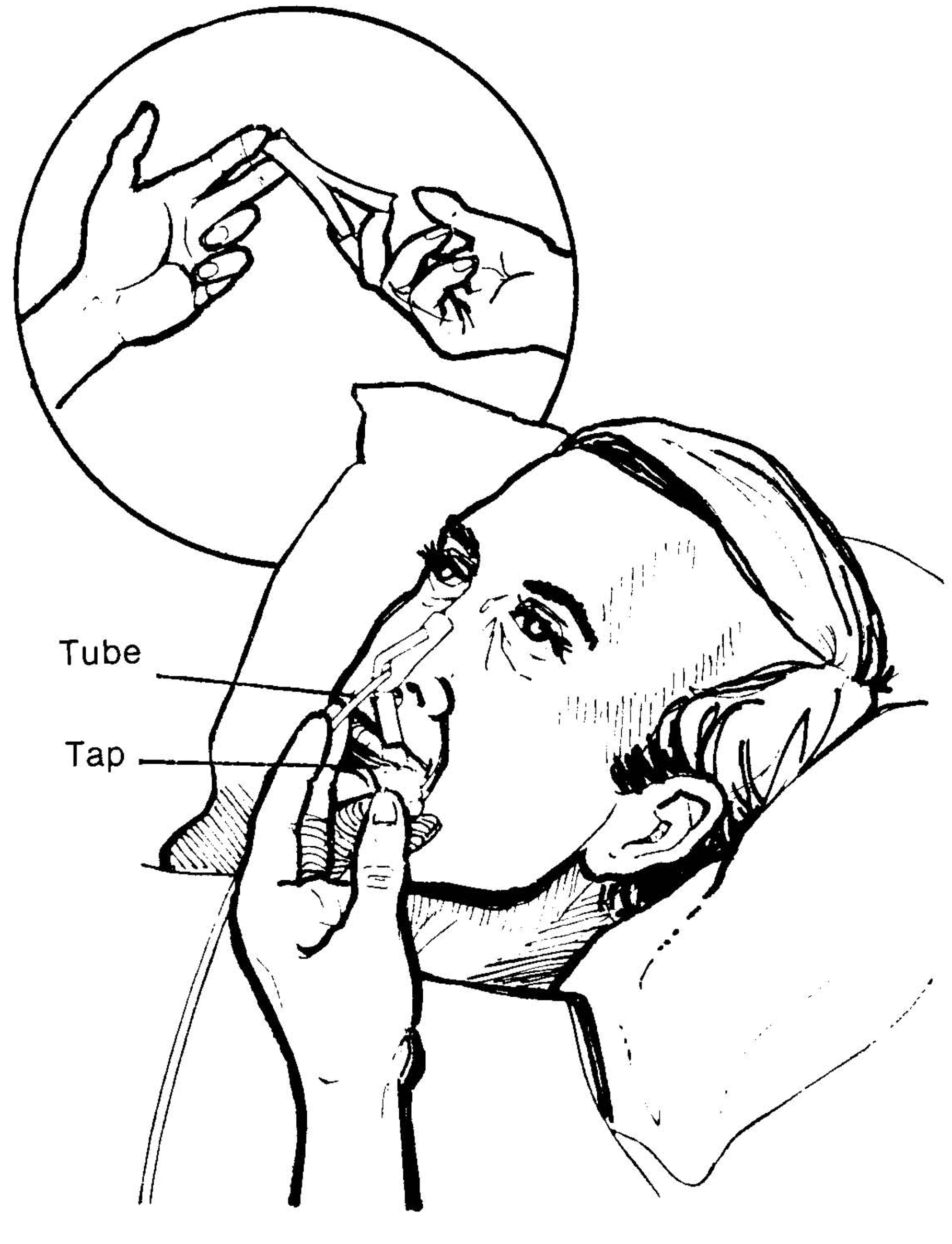
I was once taught (by a sage wise man...or was it a woman?) that upon placement of a NPA, one should secure it using a safety pin and a piece of tape to the bridge of the nose. I was asked about this and after a 30 minute search on Dr. Google, I was able to find a single reference in a Respiratory Therapy exam review textbook and one "study" published in 2008 (not able to access the actual document, only the abstract).
Two questions:
1) is this standard practice in your service, and
2) is the action of securing the NPA device part of your policies and procedures?
Two questions:
1) is this standard practice in your service, and
2) is the action of securing the NPA device part of your policies and procedures?