gotbeerz001
Forum Deputy Chief
- 1,312
- 926
- 113
#conflicted
Sent from my iPhone using Tapatalk
Sent from my iPhone using Tapatalk
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
My personal take is that the type of paramedic that most, not all, FFPM's portray is dictated by the approach their department, and in turn, culture with it takes with the EMS delivery of their department.For those who have a problem with carpenter pilots, what do you think the appropriate level of interaction should be?? I hear gripes that fire medics are lazy and chronically undertreat patients but also are not appreciated when they try to maintain or dictate care beyond field transfer. So where is the "sweet spot" for a fire medic trying to get along? I wonder if maybe some transporting medics find that they have conflicting thoughts on the matter which set them up to always talk **** about the FFPM just trying to do their job
The sweet spot would be no fire-medic at all. There is no need to have an ALS provider available for the care needed in the seconds to short minutes they'll actually spend with the patient. The only patients and interventions that are that time sensitive require BLS care. If arrival of a transport unit is so delayed that this isn't the case than that system is drastically under-resourced as for a large segment of our sickest patient, while what we do may alleviate symptoms, definitive care is only found in the hospital.
We're currently dealing with the Ontario branch of the IAFF pushing a platform of "Fire-Medics" (something we do not have anywhere in this province). They want any FF's who are currently or were once Paramedics to be able to practice as such while working as a FF. They're arguing that it's both cost neutral, which no union worth the dues they're paid would actually allow for long and that it's for the benefit of patients, despite that total lack of evidence of need. Certainly they've been arguing response time, but refusing to do an apples to apples comparison on times. Since EMS in Ontario measures from call received to arrive scene and fire reports travel time only.
I'm not saying a service cannot provide excellent pre-hospital care and provide top notch fire suppression and rescue, but when EMS is viewed as a merit badge course, and something you do to get on the engine or to keep call volumes up, etc etc. than that's not the case.
No I'm saying they shouldn't have a system so poorly resourced that a properly staffed Ambulance takes 15 minutes in an urban or suburban area for to reach a high acuity call. I work in a very well resourced area, our response times are at records lows and FD does not beat us to calls in an estimated 75% of calls (data is still pending) and when they arrive before us it is by less than a minutes. (We are station based, but dynamically deployed to balance coverage)So you're telling me that the unstable pt in a treatable dysrhythmia or a severely hypoglycemic pt should remain in their state for and additional 5-10 minutes because of "politics"?
Sent from my iPhone using Tapatalk
Good analogy except for this part does not apply to new pilotsYou are going to be flying a beautiful plane. You've got an excellent work schedule, and you're gonna make some awesome money.
")
but I find that things work best when you have both sides working together to provide care.
Not questioning your commitment or competence, or saying that your system doesn't provide good care. You asked for the "sweet spot" I think the sweet spot is no Fire-Medic, because no more than a First Responder trained FF is needed for the occasional manpower augment on very high acuity or trauma calls.While I don't disagree with you, your experiences and mine vary quite a bit. We currently (transport) cannot keep a full staff and at any point have up to 30 open spots being covered with OT and forced mandation.
Your system sounds ideal but does not match the reality that I see in both my systems. Fact is, for better or for worse, the fire medic is a necessary part of the matrix. Maybe it is because I work both sides and take my role seriously, but I find that things work best when you have both sides working together to provide care.
Sent from my iPhone using Tapatalk
While I may not like the huge push to be both firefighters and medics, I don't completely disagree with their existence as a whole. Where I disagree is like some ad I saw a long time ago regarding a cardiac arrest with 6 medics on the call and questioning what level of care people would want for their family (P vs B).
I don't have enough hours in the day to be the "best" at everything now required of ambulance personnel so how on earth you can combine the two is beyond me ....
http://emtlife.com/threads/fear-mongering.42509/I've been looking for this ad! It's a laughable one from both a system design and a clinical perspective...
Just saying every one of those dudes is jacked beyond belief lol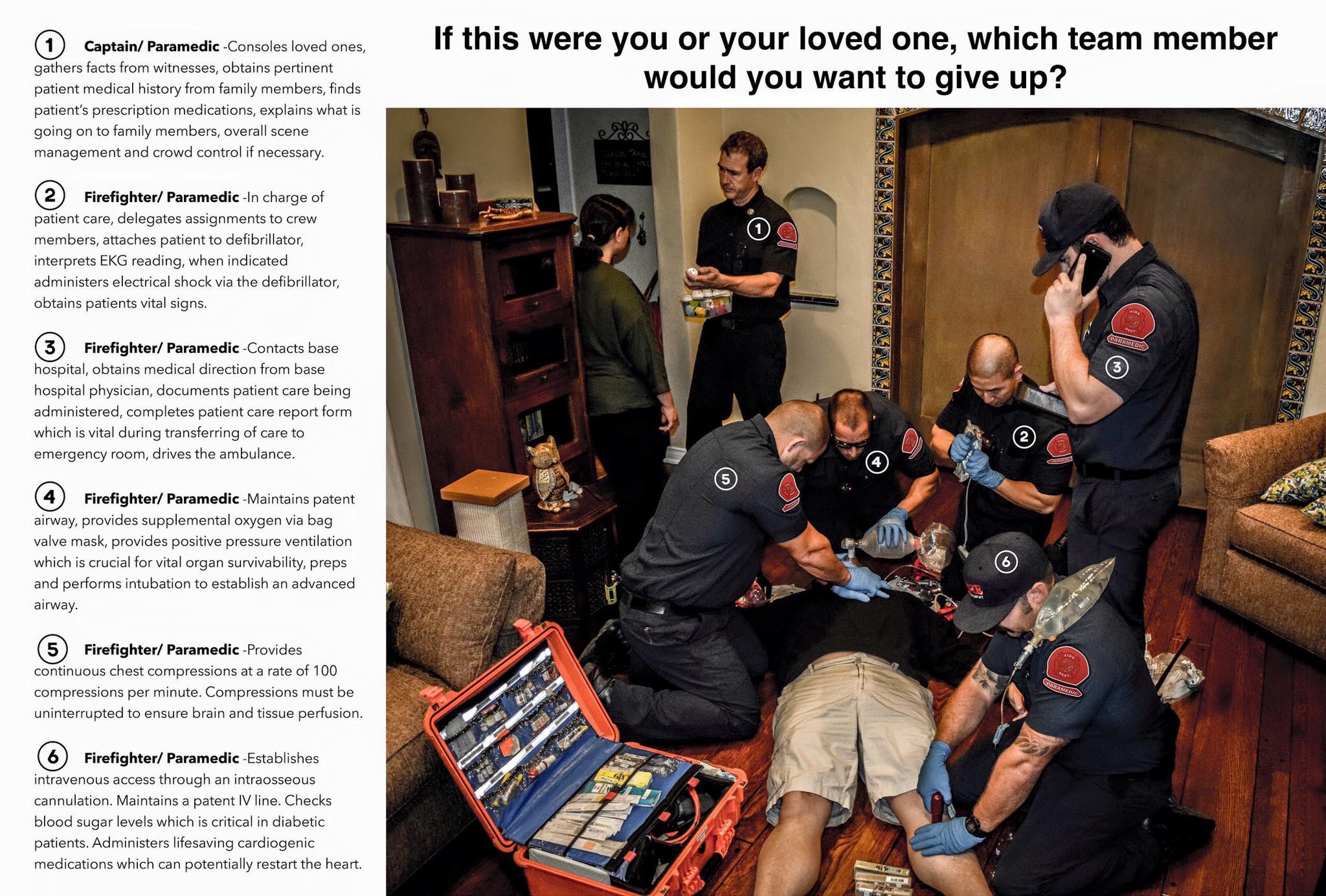
@DEmedic
This is the greatest picture ever.
Who knew that you needed a paramedic to perform chest compression...?
Just saying every one of those dudes is jacked beyond belief lol