jedirye
Forum Lieutenant
- 114
- 0
- 0
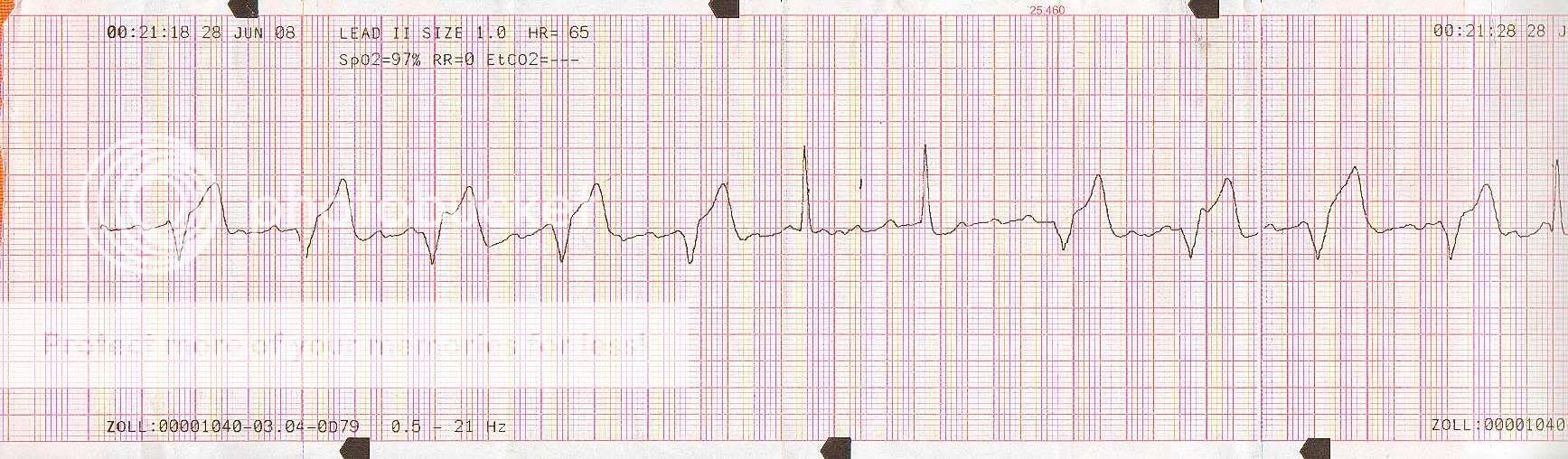
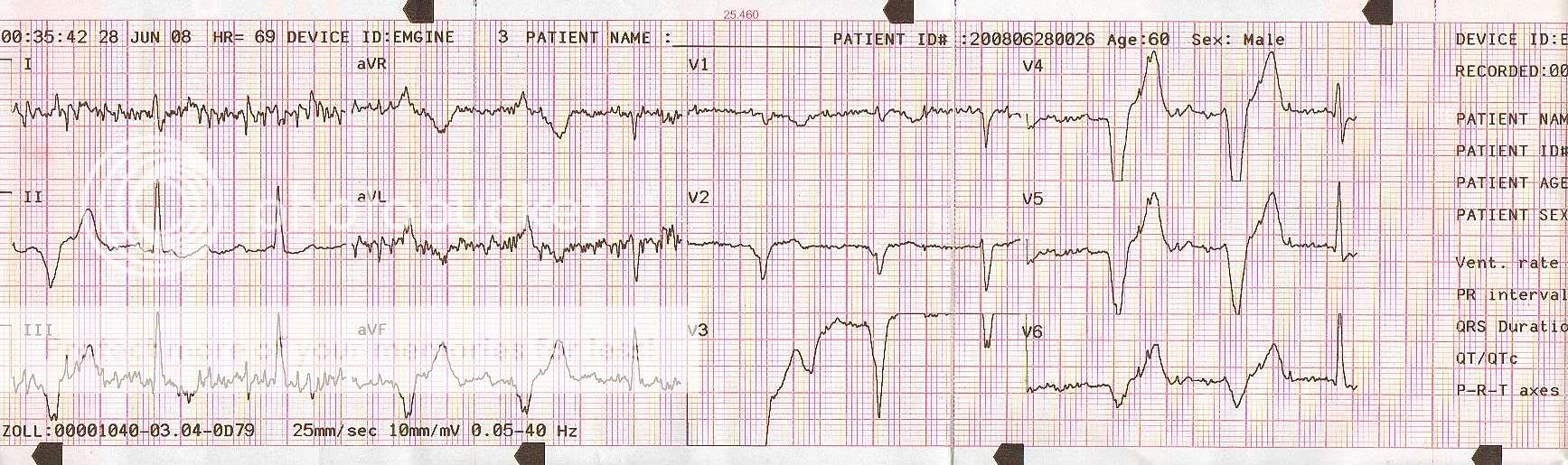
So I'm on a clinical and around midnight or so we get called for an OD. Guy is a 79 Y/W/M pt who intentionally ingested an unknown amount of hydrocodone (prescription x 2 years ago) to intentionally hurt himself. Pt is found sitting by toilet dry heaving, nothing in bowl (no pill fragments, etc.) Pt is A/Ox4 with a GCS of 15. Pt ingested the unknown amount (bottle stated 20 pills) over the course of three hours. Get him in the truck, hook him up and I see that crazy rhythm. Hx of patient? Pacemaker, yes, but I see no pacer spikes on the strip. Pt also had an ablation done for I believe tachycardia. Pt denies any cheif complaint at the time other than N/V (no chest pain, SOB, etc.) All complexes are perfusing, by the way. I'm riding with a seasoned vet. who looks at the screen and says no big deal. I insist on doing a 12-lead regardless and the one included was the best I could get (and that was with the truck stopped!). I brought this strip into work with me to see what other medics had to say because I am still baffled by it. No one has given me a definitive answer. I brought the strip with me to the next clinical and asked the seasoned vet. what he thought it was as well. He gave me some round-a-bout answer and didn't really give me a definitive answer either. Any takers??
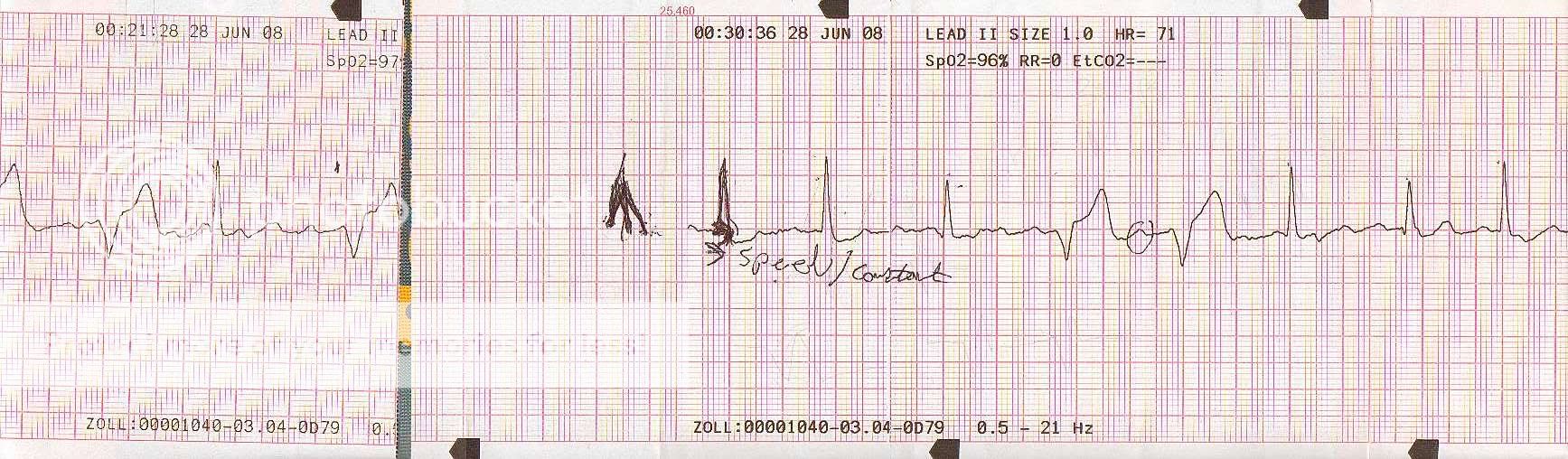
Also, pardon the writing, the seasoned vet marked my strips! :glare:
Appreciate any insight and help. I'm still learning here (and forever will)...
-rye
Also, pardon the writing, the seasoned vet marked my strips! :glare:
Appreciate any insight and help. I'm still learning here (and forever will)...
-rye
")