joedittfurth
Forum Ride Along
- 7
- 0
- 0
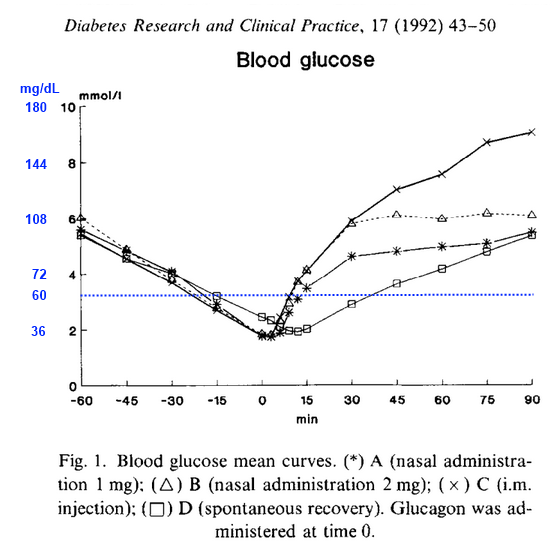
anybody out there have any insight on nasal atomizers specifically with glucagon
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
with any tool, they have their place.
I.E. the seizing patient that you are going to have a hard time getting an IV on. wanna break that seizure. with Valium
Cardiac arrest where narcotic toxicity is the suspected cause
just because you got the NAD dosent mean it fits every patient.
with any tool, they have their place.
I.E. the seizing patient that you are going to have a hard time getting an IV on. wanna break that seizure. with Valium
Cardiac arrest where narcotic toxicity is the suspected cause
just because you got the NAD dosent mean it fits every patient.
If you've never given it, and only seen it one, how can you form an opinion?
I use IN Narcan exclusively now for Opiate ODs. I have had excellent results with it. I find that Versed is hit or miss, depending on the concentration I have in my box. Fentanyl IN works great for kids, but I find IV Fent better for adults.
")
with any tool, they have their place.
I.E. the seizing patient that you are going to have a hard time getting an IV on. wanna break that seizure. with Valium
Cardiac arrest where narcotic toxicity is the suspected cause
just because you got the NAD dosent mean it fits every patient.
anybody out there have any insight on nasal atomizers specifically with glucagon
Really? Why is that? Our IN dose is 1mg.
Interesting. I'll share that with the guy in our Protocol Revision group. I'm sure they'll just say, "continue to give 1mg IM" however.