CCCSD
Forum Deputy Chief
- 1,977
- 1,255
- 113
All I know is my surgery got cancelled…so I’m back eating narcs like candy.
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Shouldn't that statement apply to both sides of the discussion?However, you shouldn't base your judgement on what is happening elsewhere based on what you see in your hospital. If you haven't seen what happens when the number of staff out doubles every two days and that goes on for 10+ days... well... all of a sudden 10 days of iso doesn't work and it can become a contingency situation or a crisis.
I encourage you to reread my post: I acknowledged I don't know what is happening in his one hospital. But I do know what is happening in dozens of other hospitals.Shouldn't that statement apply to both sides of the discussion?
I read and understood your post. I was pointing out that you're willing to base your judgement on what other locations should be doing based upon what you've seen in your systems while calling out others who are making their own judgements based upon experiences that are different than yours.I encourage you to reread my post: I acknowledged I don't know what is happening in his one hospital. But I do know what is happening in dozens of other hospitals.
I was quite clear that:I read and understood your post. I was pointing out that you're willing to base your judgement on what other locations should be doing based upon what you've seen in your systems while calling out others who are making their own judgements based upon experiences that are different than yours.
how concerning is it that both @Carlos Danger and I are in complete agreement on this? Could this be a sign?I'm totally OK with that, of course, if that's what the science tells us makes sense. The problem is that it's completely inconsistent with much of the other things we are still being told.
The pandemic is no longer an emergency and even though the public health authorities definitely won't admit that because all their power is dependent on the public being fearful, it appears that they are finally to the point that they will at least balance their interests against the costs of the policies that they espouse. I'm sure it's totally coincidental that this is happening at a time that the approval ratings of the sitting administration are plummeting and midterms are only 10 months away.
Hospitalized with COVID, or hospitalized due to COVID? Because those are two very different numbers; the former is ehhh, the later is emergent. Even the CDC is now admitting there is a distinctionHere in Tennessee, we averaged 13.5K infections per day last week. About 2700 Tennesseans were hospitalized with COVID as of Sunday.
Can you imagine what would have happened if the previous administration had done this? the public outcry, the news media condemning the administration for not caring about the lives of people, the death counter skyrocking and running 24/7.... it's almost like the response isn't based on science, but politicsHowever, you shouldn't base your judgement on what is happening elsewhere based on what you see in your hospital. If you haven't seen what happens when the number of staff out doubles every two days and that goes on for 10+ days... well... all of a sudden 10 days of iso doesn't work and it can become a contingency situation or a crisis.
I mean, hospitals fired staff who refused to get vaccinated.... if it was an emergency, you would think they would have allowed them to keep working, so they could staff the hospital... right?So if you had enough staff sick at once that you couldn't staff the hospital... due to the pandemic... that they have to work while contagious... emergency or not?
The previous administration did do "this!"Can you imagine what would have happened if the previous administration had done this? the public outcry, the news media condemning the administration for not caring about the lives of people, the death counter skyrocking and running 24/7.... it's almost like the response isn't based on science, but politics
What I think most people who don't spend their time looking at epi curves and occ health data for multiple multi-hospital health systems do not understand is how unbelievably fast this crisis happened, but not everywhere at the same time. It is truly unbelievable to watch from the standpoint of hospital epi. I have never in my life seen anything move so fast. Case doubling rates of ~2 days. Most people just cannot fathom that. Probably 10-20% of people in a community having Omicron at the same time! I can't be surprised because I literally watched the foreign data and watched it come my way first and tried to warn the system 4 weeks ago. It struck some mountain tourist areas first and very hard. The metros lagged... but now they are getting shellacked. The only good news is this will all be over quickly (weeks instead of months with past waves).I mean, hospitals fired staff who refused to get vaccinated.... if it was an emergency, you would think they would have allowed them to keep working, so they could staff the hospital... right?
did what? told healthcare workers to return to work while still covid+? shortened the quarantine period from 10 days to 5, due to business demands? Can you please cite a source that said this? Because otherwise, I am going to have to call BS on this. After all, it was the NY and NJ governors who places covid+ seniors with healthy ones in nursing homes (the federal government only said to do that if you would keep them safe and separated, a section which the NY governor neglected to follow).The previous administration did do "this!"
Riiiiiiiight. I mean, it's not like the administration or the CDC is changing the guidance, and the hospitals are following it.The guidance was there for crisis return to work (working while positive). I've covered this in my previous post. There are reasons it wasn't activated BY THE HOSPITALS.
Crisis RTW isn't some new Oval Office led standard. The Crisis lane was there this year, last year, and in 2020. It is the situation on the ground that led hospitals to activate it or not... not orders from the Oval Office.
did what? told healthcare workers to return to work while still covid+? shortened the quarantine period from 10 days to 5, due to business demands? Can you please cite a source that said this? Because otherwise, I am going to have to call BS on this.

According to The Tennessean, the principal daily newspaper in Nashville, approximately two-thirds of the patients were admitted specifically for COVID. The Tennessean adds that there are 12,000 new COVID infections per day, as of last Friday. They also point out that the more immediate crisis is the scarcity of hospital staff, due to infection and quarantine, and that hospitals could be overwhelmed if COVID cases continue to climb and staffing continues to drop.Hospitalized with COVID, or hospitalized due to COVID? Because those are two very different numbers; the former is ehhh, the later is emergent. Even the CDC is now admitting there is a distinction
I share your concerns, but I think U.S. public health standards and practices are going to have to be redefined to allow for a society that is less willing to follow relevant directives than they were, say, 60 years ago. In my opinion, perceived dangers of expedited COVID vaccines are mostly excuses for non-compliance. I believe the real reason is an inflated sense of "rights" to do and not do as we please.My understanding is that the C-19 Omicron variant is the nearly the most virulent infectious disease we've ever discovered, only being surpassed by measles. Unfortunately, that means that nearly everyone is going to be infected and quickly, so I understand why the return to work protocols are in place.
A new variant that is similarly infectious but is as deadly as prior variants would be a nightmare scenario. High rates of vaccination and committing to population wide infection control for several years is going to be necessary for us to get ahead of this.
Measles and smallpox are nearly forgotten. It's possible to do it.
No, I am not missing any point at all, I know this isn't what you and your ilk intended. I understand that it isn't what is supposed to be happening. But it is the predictable net result of policies that you vigorously support: Contribute to a staffing crisis by firing (unvaccinated) workers because they might come to work with COVID; then, because we are short staffed, amend the guidelines so that workers can come to with with COVID. That's what is happening. It is happening (at least partly) because of polices that you supported. Own the consequences of your decisions.You are missing the point entirely. That is not what is supposed to be happening. If places are choosing to do crisis staffing without a crisis need, they are NOT following the intent of the guidance. Sounds like a hospital failure based on greed, not a public health guidance failure.
I am not putting words in your mouth; at least, certainly not any more than you do to me. I am simply saying that if you espouse these policies, then you own their logical extensions. You have repeatedly supported the idea of firing non-vaccinated healthcare workers. Fine. In a vacuum, that makes sense. But now you are supporting having COVID+ healthcare workers come to work. That does NOT make sense, at least, not in light of your previous positions. I know, I know....you are going to bring up the fact that vaccinated people are LESS LIKELY to acquire or transmit the virus. I get that - I really do. But in continually banging that drum, you are completely ignoring the facts that 1) many of those fired workers HAVE natural immunity comparable (or better than) the immunity conferred by vaccines, and 2) vaccinated people still acquire and transmit the newest variant at a very significant rate. Any way you slice it, I don't see any way to support having people come to work who DEFINITELY have COVID when you also supported firing people because they MIGHT come to work with COVID. Do you really not see the logical disconnect there?Are you seriously putting those words in my mouth?
No, I'll wait for YOU to explain what is "conspiratorial" about anything I've said here. When you can't - and I know you can't because there's nothing conspiratorial at all about the idea that federal guidelines are very often politically motivated - then it'll be obvious that this statement is nothing more than an ad hominem. I guess it's a good thing that "not disappointing Summit" isn't very high on my priority list.I'll just wait for some more of your conspiratorial thinking that this is all about power, politics, and control. You disappoint me.
")
Ahhh, no. First of all, you aren't the authority on what is "right", neither is the sitting presidential administration. Secondly - right or wrong - there is overwhelming precedent in our culture about the primacy of the individual vs. the collective. This is the main thing that separated the US from the rest of the world, both culturally and politically speaking, historically. So don't act like the fact that almost 75% of our population being vaccinated in well under a year somehow represents some never-before-seen level of selfishness. In fact some would argue the exact opposite.People often confuse having a right with doing what is right.
What is new is a widespread reaction to being informed of what is right: a pathological determination to exercise the right not to do what is right. Toddlers excel at this. It is sad to see such juvenile behavior cast as virtuous for adults.
Presumptuous? Arrogant? Lol. If that isn't the pot calling the kettle black, I don't know what is.Me and my ilk? Yea. You don't just disappoint me. Your disingenuous, inflammatory, presumptuous, and arrogant posts frankly disgust me.
I won't hold it against you. That's what folks do these days who don't like hearing from those who disagree with them. I wish you luck with that.That's as much as I can say within the bounds of the rules of this forum. I do wish I could say more. But I can't, so I think I'll check out this neato ignore feature. I have appreciated you over the years on other topics, but you really aren't worth my attention anymore. What a shame.

How does your epi curve show hospital staffing levels and admissions? From what I can see of it, it only shows new cases, not cases admitted to the hospitals. Yes omicron is more infectious, but a lot of the infected are already vaccinated and as you have so often said, vaccination means reduced hospital admissions and disease severity.'memba when CDC shortened quarantine under the last admin? https://www.cdc.gov/coronavirus/201...tific-brief-options-to-reduce-quarantine.html
I 'memba.
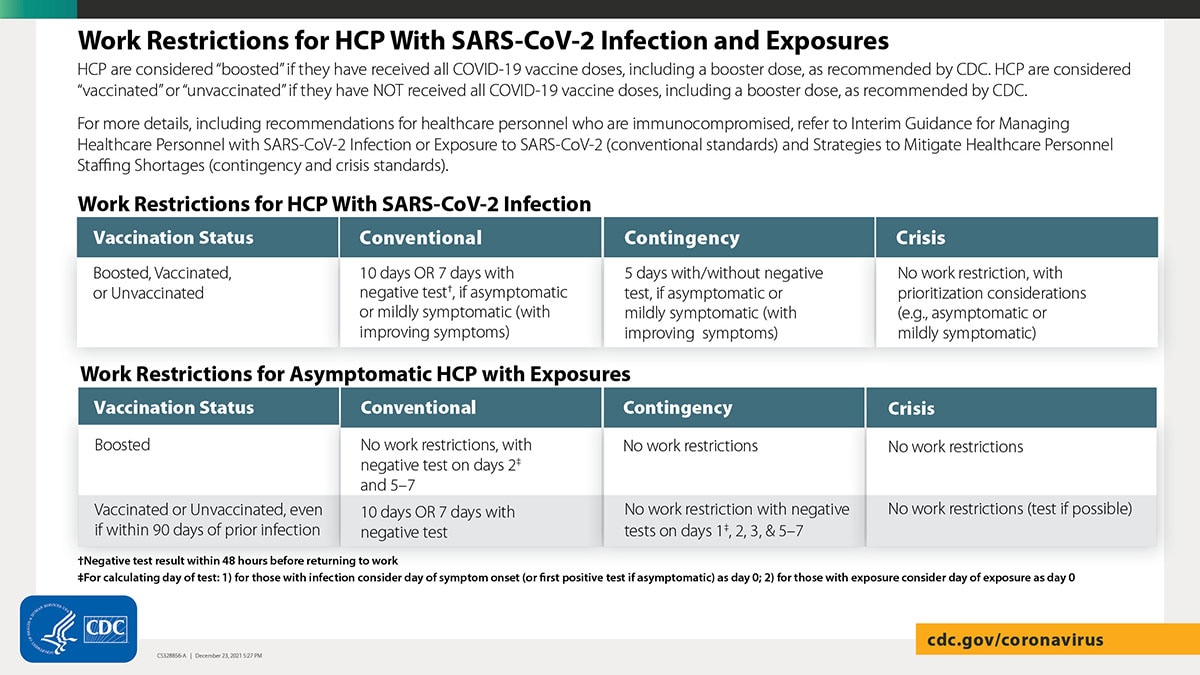
Look, you have to remember there are multiple "Lanes" for operations based on the staffing shortages vs surge. If things are fine you don't have to get drastic. Here is the newest emergency guidance that was released knowing that Omicron was imminent:
That CRISIS lane was there before the current admin in previous guidance! That is NOT BS. Carlos even agrees with that.
The benefit of having enough nuance to add the middle contingency lane is this: it gives you somewhere to go BEFORE Crisis, and knowing that max shedding is -2 to +3 days from sx onset, and knowing that almost all your HCPs are vaccinated and have shorter shedding time, you can make calculated risk benefit decisions.
You might also want to take a look at this epi curve. It shows the entire pandemic. Do you see how the Omicron case surge is dwarfing everything ever before? IT IS DOING THAT TO HEALTHCARE STAFF TOO! How would YOU handle the current situation?
View attachment 5464
Remember: the guidance was NOT "everyone go to contingency and crisis because you feel like it" as you seem to suggest. Not at all. But what if you end up with so many staff out that you can't care for your patients without moving to contingency? Or Crisis? What should you do?
It's easy to point fingers and blame politics when you just come in and do your individual job for your handful of patients. But when faced with the stark realities of the situation across a department, hospital, system, nation, what would YOU do?
And if you answer is drop vaccine mandates, you may as well not post it because getting a 1% increase in staffing is not the answer to the curve above.
Yep, you're now the proud owner of an ilk.Me and my ilk?
 I used to have one around 1970. It's sort of like an imaginary friend, with someone else doing the imagining.
I used to have one around 1970. It's sort of like an imaginary friend, with someone else doing the imagining.I absolutely understand your point and I think I wasn't clear in my point. The hospitalizations are up, but not so drastically as to be causing the crisis by itself. The point I was making is that it is about sick staff and you do NOT have to be hospital sick in order to be too sick to go to work, or to be restricted from work.How does your epi curve show hospital staffing levels and admissions? From what I can see of it, it only shows new cases, not cases admitted to the hospitals. Yes omicron is more infectious, but a lot of the infected are already vaccinated and as you have so often said, vaccination means reduced hospital admissions and disease severity.
Maybe that 1% of fired employees would be the difference maker in avoiding critical staffing shortages? I'd be interested to see any factual evidence or studies on this, but to date there doesn't appear to be any.
And now the CDC admits that vaccinated people might have more problems with developing resistance...it's getting to where we can't trust anything because it changes so often and not just a small shift but a 180 degree turn.and the cases of vaccinated people becoming covd+ has blown up.