bigbaldguy
Former medic seven years 911 service in houston
- 4,043
- 42
- 48
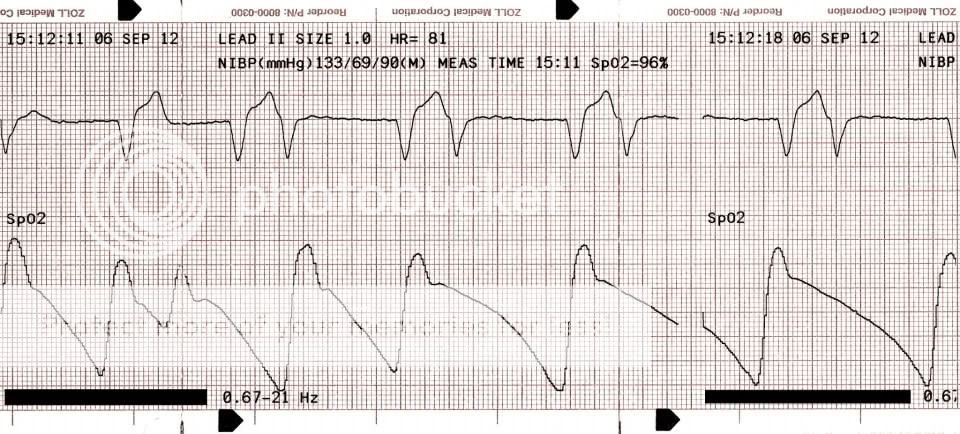
What do you think.
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Without a 12 I'd call it IVR with PVCs.
Just my .02

Don't sell yourself short! Your interpretation is worth at least a nickel
Oh and BBG stop stealing stuff of Facebook
Score!!!!
One thing I will say is if those, in fact, are PVCs they are reasonably close to the T wave and I'd be watching real closely for any R-on-Ts or movement in that direction. This has potential to go south quickly if it already hasn't. I'd love to know the patient's presentation.
I personally don't think it's paced. I'd think you'd see pacer spikes even in a single lead but I'm also new as heck at this medic thing so take that for what it's worth.
Akula, and Chase for that matter, I'm not sure I'm seeing this 3rd Degree AVB you both speak of. I do agree that the baseline looks like it has potential to be A-fib or was at one point recently before this disaster of a rhythm started.

I do not think this particular rhythm is paced but it would be on my differential to rule out. Sometimes pacer spikes can be very hard to see. With a 3rd degree AV block you have an atrial rhythm as well as an underlying escape rhythm which is usually junctional or ventricular. And IVR is basically just a ventricular rhythm without atrial activity. The most common atrial presentation is sinus, the multiple P waves, however you can also have atrial fib as the underlying atrial rhythm. This presents looking like a bradycardic wide complex ventricular rhythm which is very regular (Ruling out A fib) with atrial fibrillation inbetween the QRS complexes. So basically looks like IVR but with a fib inbetween instead of a straight isoelectric line. There is a complete AV block with the atria and ventricles doing their own thing. Or something like that, I am just getting off a night shift and am sleep deprived.
Its fun watching patients with frequent PVCs on the monitor who also have an A-line. You can see the decreased cardiac output, if any, with the premature beats.
Ok, I see what you're gettin' at. I was so set on the picture perfect 3AVBs I've seen in books and the one and only that I've had in the field that was textbook looking. That makes sense though.
Dude, I like to think of myself as being decent at interpreting ECGs but you run freaking circles around me.
What do you think.
Or a BSN about to graduate...but hey whatever way you like it hahaha
FWIW I'd almost be inclined to call that A-flutter but then again in other leads it's definitely A-fib.
That was something that caught my eye as well. If all was functioning as it should, SpO2 waveform should occur normally just "after" or to the "right" of the QRS complex that results in a perfusing beat. Some of those waveforms seem to occur after the first complex in the pair, some occur after the 2nd complex in a pair.The SpO2 waveform does not look contemporaneous with the ECG which seems odd.
What do you think.
The squigglies aren't squiggling right.
Here is a crappy example of a 3rd degree AVB with a junctional escape and underlying A Fib. Some of the leads look like A flutter so just ignore those lol (From Lifeinthefastlane)
The SpO2 waveform does not look contemporaneous with the ECG which seems odd.