zmedic
Forum Captain
- 480
- 0
- 16
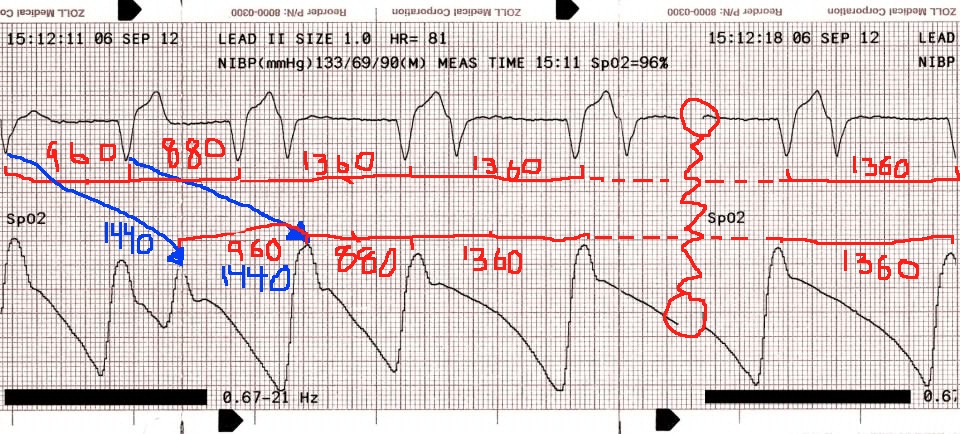
Also the QRS is getting pretty wide. Maybe it's PVCs or a ventricular rhythm, but I would worry about things that widen the QRS like TCA overdose or hyperkalemia. It's getting a bit sine wavey.
But the big thing is if you are going to look at a rhythm strip you should have 3 leads, and a longer strip, like 6-10 seconds worth, or a QRS. One lead is basically "is this Vtach/Vfib?"
")