VentMonkey
BS, FP-C, CCP-C
- 5,788
- 5,128
- 113
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
I probably shouldn't say what my first thought to this was....Yup.
I probably shouldn't say what my first thought to this was....
EMT here. NJ though so I can't do IV's. This is a BLS call so honestly we can put you on the cot in your comfortable position and secure x3. Transport as comfortably as we can .. this isn't really a medics situation for us, but they pay be interested in doing pain management ...otherwise they'll just release.
*edit*-- would probably need medics for pain management -- missed the 20 min transport time, my l1 trauma center is 5 minutes away.
Sent from my LG-H810 using Tapatalk
5'11-6' 180-185How much do you weigh? Height? Figure out my dosing from there...
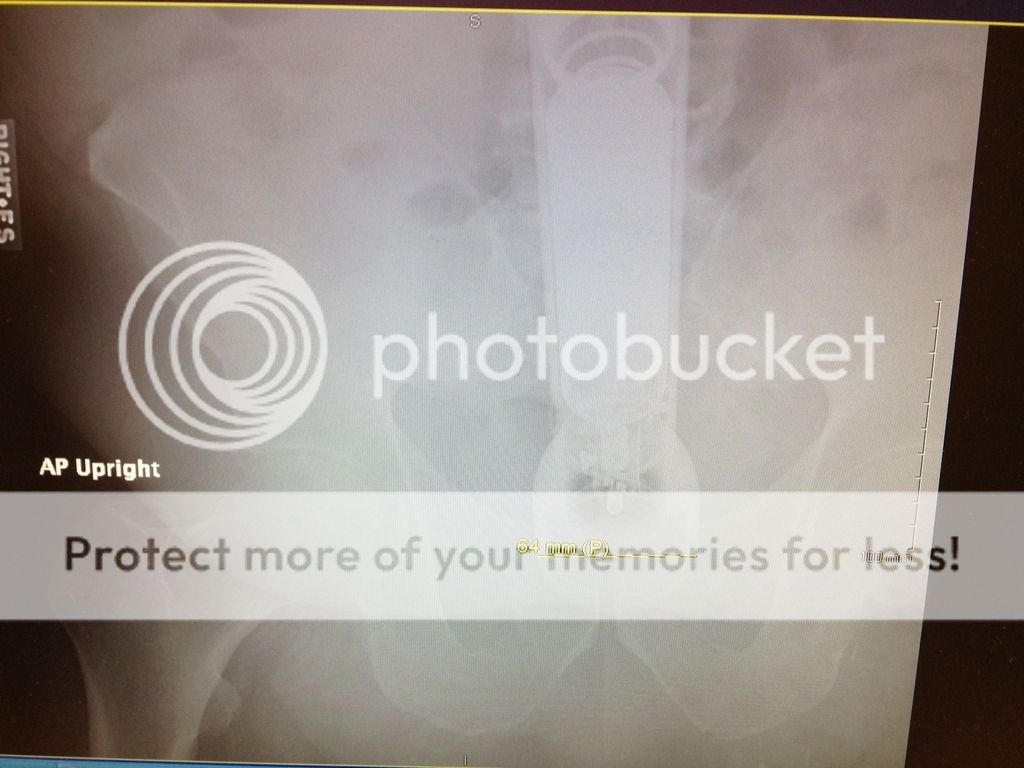
Not quite. It was they took the saying "anything is a dildo if you are brave enough" as a challenge.If your first thought was maglite, then you are correct.
Not quite. It was they took the saying "anything is a dildo if you are brave enough" as a challenge.
5'11-6' 180-185
")
ahh.. close, but no cigar, And thank you for catering to my needsNo lights or sirens for you.
IV, 150 mcg of fentanyl q 10 PRN. 4-8 mg of zofran PRN. 25mg of da ketaminez if the fentanyl doesn't make you stop squirming and whining so I can chart in peace
Pylo, ischemic bowel and obstruction are high on my list.
Sent from my iPhone using Tapatalk
lolBecause that always solves marital conflict. He must have been pretty mad....and well practiced lolGood point but in this case it was "I was mad at my wife so I did it to show her how mad I was."
"Sir, was there alcohol involved?"
"Yup."
Normal sample history,what exactly the PT had before hand and when exactly the pain started and in what way.much of which was answered already but I can't do pain management IV's or anything. We do have is have abdominal pain, previously treated, id check for any masses but if I did find something it isn't any immediate relief to the pt. Just more info for the nurse. So transport is the best bet. No lights.Before we jump to treatment, what other things do you want to know? What is on your differential?
You are called to the residence of a 26 year old male, who is having debilitating abdominal pain.
Background on the patient: seems to be physically in shape, is currently on the floor in the living area of the house curled into a ball. Patient states that he has been having moderate to severe pain for 2 days, on the left side of his abdomen, radiating to the lower left back.
Pain on scale: 11/10. Pain described as: stabbing, stomach turning inside out, and burning. Last oral intake: about 4 hours ago/ few slices of bread, patient states he could not eat due to pain increasing upon intake.
FFW: patient is now in the ambulance, 20 minute transport time to a level 1 hospital has any capability (closest and obviously best choice). V/S BP:150/90 RR: 20 Sat:98% HR:96 SR
Patient also states he is not allergic to any medications to his knowledge.
curious as to: 1. How do you transport this patient(LS or non emergent) 2. Pain control? 3. General impressions? 4. what other information would you try to gather?
Appendix is on the right side of the abdomen (i was taught to do rebound pain test on LRQ to test for appendicitis), if im not mistaken (i probably am..), abdomen is rigid to an extent, not rock solid, but not "normal" no nausea, no vomiting. Urination normal, stool present but bloody. no trauma, only the past day- to 2 days.Differentials...appendicitis, pyelonephritis, pancreatitis, urolithiasis, peritonitis, bowel obstruction...
+ CVA tenderness? Is the abdomen rigid, supple? Rebound tenderness? Nausea? Vomiting? Normal ins/outs (eating/drinking and urination/defecation)? Any trauma? Has this happened before? I'd like to get a quick social history, too - ETOH, namely.
Patient cannot move, cannot stand, can roll over, but causes agonizing pain.Ideally, I'd get V/S in the house. Can the patient walk? Do we need to assist him to a standing position? Or do we have to lift him to the stretcher? If need be, I'd rather get ALS on scene for pain control prior to moving him. If this is too time consuming, it's easy enough to move this patient (not particularly heavy).
Appendix is on the right side of the abdomen (i was taught to do rebound pain test on LRQ to test for appendicitis), if im not mistaken (i probably am..), abdomen is rigid to an extent, not rock solid, but not "normal" no nausea, no vomiting. Urination normal, stool present but bloody. no trauma, only the past day- to 2 days.
Patient cannot move, cannot stand, can roll over, but causes agonizing pain.
What everything actually was will be put up later today.
). .
.I very rarely transport anyone other than the patient. If your girlfriend is able to drive herself to the ED that is overall going to be the better optionrefused to transport my girlfriend with me for some reason.
