Shishkabob
Forum Chief
- 8,264
- 32
- 48
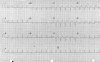
Holy cow, did they have the patient jumping around while analyzing the 12-lead?
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
....along with the fact that we should treat the monitor and not the PT.quote]
Um, I'm pretty sure the saying is the other way around. Which may go a long way in explaining why they did what they did.
Yes, once an MI has been established via 12 lead and labs the pt needs to be treated for it regardless of the exact symptoms they are feeling. However, you should never treat the monitor and ignore the patient. Morphine is included in the MONA cardiac protocol, but would you automatically give it because there is a MI on the monitor even if your patient isn't in pain?
You are acting totally shocked and surprised that they treated for respiratory. Without the 12 lead, respiratory is part of the differential diagnosis. Yes, diabetic females usually present atypically during MI/Cardiac events, but you have to remember that diabetic females can also have respiratory problems without it being an MI.
Smoking leads to respiratory problems just as much as it leads to heart disease. You can't use smoking to rule out anything, just to increase your suspicion for certain disease processes.
But, this should've been recognized without a 12 lead. There were multiple factors which scream out AMI along with the fact that we should treat the monitor and not the PT.
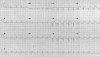
The first 12-lead ECG taken in the ED is suspicious, but it isn't an obvious STEMI. It's apparent the ED physician on duty didn't think so either. So what we have here is a prehospital 12-lead ECG with poor data quality. Not exactly a shocker, and certainly not evidence that fire-based EMS sucks. Frankly, I'd be more concerned about why the ED didn't perform serial ECGs or continuous ST-segment monitoring with poor R-wave progression and broad-based T-waves in the precordial leads. Must have been a fire-based emergency department.
:excl::excl::excl: Oh :blush: I sure am dyslexic. It it was a typo. I meant to say treat the patient and not the monitor :excl::excl::excl:
")
Why do serial ECGs when hospital labs can get some labs results within 5 - 10 minutes? EDs are not going to wait for an ECG to look text book. Ever hear of non-STEMI MIs?
ECGs are not always the definitive and only diagnostic that is done.
The hospital arranged for transport to a more appropriate hospital. Would you prefer the doctor admit the patient to tele until the ECG was perfect just like in the text book or the patient coded?
Some Paramedics do get hung up on wanting the "STEMI" and miss other important signs or symptoms especially in a patient such as this who presented with the risk factors and signs/symptoms.
In the last several posts absolutely NOTHING was mentioned about fire-based EMS. You now seem to have something to prove that your department is perfect and know it all already. Get over it. Again, when you force FFs to be Paramedics, not all will be good or even barely adequate at that job. Being a FF is not what will help you learn the medicine to effectively treat a patient. Do you think you can stop with the FF stuff long enough to look at this scenario as a health care professional?
Don't take me so seriously, VentMedic. I've held my fire through numerous (and ridiculous) fire-based EMS bashing sessions and I'm just having a little light-hearted fun. As for the ECG, of course I've heard of NSTEMI, but we generally don't rush NSTEMI to the cath lab, and we certainly don't give thrombolytics. The treatment is different.
I never said anything about POC testing. Hospital labs are available 24/7 and in smaller hospitals some are within a quick walk of th ED.Point of care cardiac biomarkers are interesting, and I'm aware of emergency departments that incorporate them into critical pathways, but apparently that wasn't the case here. Even if it was, without the ECG showing STEMI, there would be no reason for immediate transfer PCI.
As for my own department, I don't think I've ever mentioned it on this bulletin board. Regardless, there's no reason that people who dish it out on a regular basis shouldn't be able to take it, especially when I'm taking friendly jabs and not foaming at the mouth.
That is patient dependent and you certainly can not make a blanket statement about them not going a cath lab.
I'm not talking about what the EMS team will do. I am talking about what the ED and cardiologist might do.
If it is a NSTEMI, you might not be able to call a "STEMI ALERT" as a Paramedic.
However, if signs/symptoms are present, going to a more appropriate facility with appropriate diagnostics could still be considered.
And correct, very few U.S. EMS agencies can give thrombolytics.
I never said anything about POC testing. Hospital labs are available 24/7 and in smaller hospitals some are within a quick walk of th ED.
Friendly jabs? You are now taking shots at thrashing the ED to make yourself look good.
Private EMS wasn't enough for your "jabs".
If you want to talk Firefighting there are plenty of forums.
If you want to discuss medicine, you don't have to be a FF to do so.
If a FD or any agency is not aware of its flaws, then it will not improve. Look within your own walls before thrashing others.
Show me the evidence that NSTEMI patients benefit from immediate PCI.
Pre-hospital really suspect that they failed to properly clean/scuff the skin leading to a bunch of artifact. I see it way to often even with the non fire EMS. Wiping with an alcohol pad is not enough but is better than many who just place them over hair, dirt and all.
To do it right you need hair shaved, wipe the skin, then scuff it. Use something like 3m red dot skin prep. A dry 4x4 does not scuff enough.
http://www.medexsupply.com/products/pid-34060/3MRedDotTraceSkinPrepRollwithD.htm
The next cause sadly is often the cables are not fully connected to the machine. I have gotten into an ambulance and medics had artifact and I just reached over and pushed cable connector further into its socket and amazingly got a clean 12/15 lead.
Another common cause is the cables developing cracks. A busy service really should replace the cables every few months, while a slow rural service might need to replace every 1-2 years.
And yet another problem especially with older machines is electrical interference. With some machines you really needed everything off in the ambulance.
Thats just a small list of causes.
I once helped with skills at a medic class and was told by the students that an instructor told them to give everyone SOB Albuterol and if it didn't work give them Lasix, because it must be pulmonary edema.