I know phlebotomy requires a particular "order of draw" for drawing blood via venipuncture. Here is the order from top to bottom according to one source.
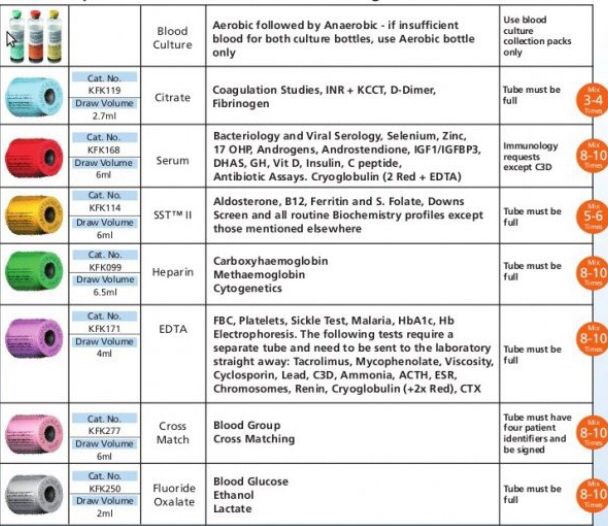
I believe EMS uses only 5 or 6 for blood draws.
Could anyone clarify which ones are utilized for the blood draw kits in EMS, and confirm which order they are to be drawn in?
I believe EMS uses only 5 or 6 for blood draws.
Could anyone clarify which ones are utilized for the blood draw kits in EMS, and confirm which order they are to be drawn in?