VirginiaEMT
Forum Lieutenant
- 247
- 0
- 0
How important is it to be able to determine left or right axis deviation in EMS? Why?
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
Useful for things like determining VT vs abarent conduction
...but Axis is useful for determining a ventricular focus (extreme RAD, for example) versus a supraventricular focus with aberrancy...
 <_<:wub:
<_<:wub:SameWe are not taught about L/R axis in our 12 lead training. A few people teach themselves. Ill probably have a look over in the future.
the lifepak 12 will tell me anyway right? ^_^
VT will have an extreme right axis which is useful in ruling it in...
VT can have any axis, even a normal axis (albeit rare)!
Interesting....that is the first I have ever heard of it. I was taught that a wide-complex V-tach is going to always have a extreme right axis. This and being able to measure the nader point assist in differentiating it from say SVT with abberancy.
Please....explain?

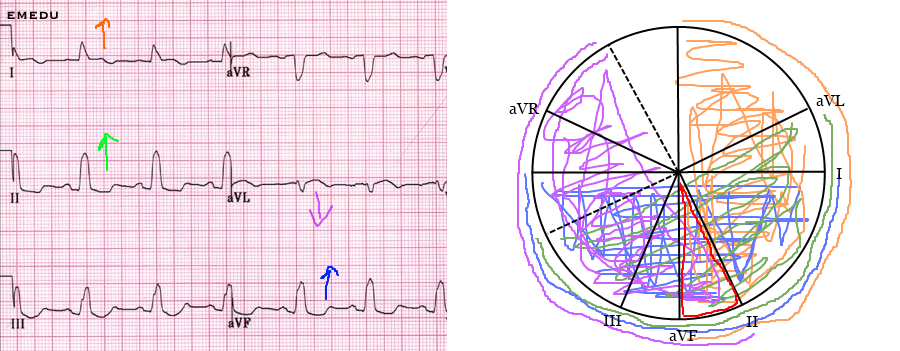
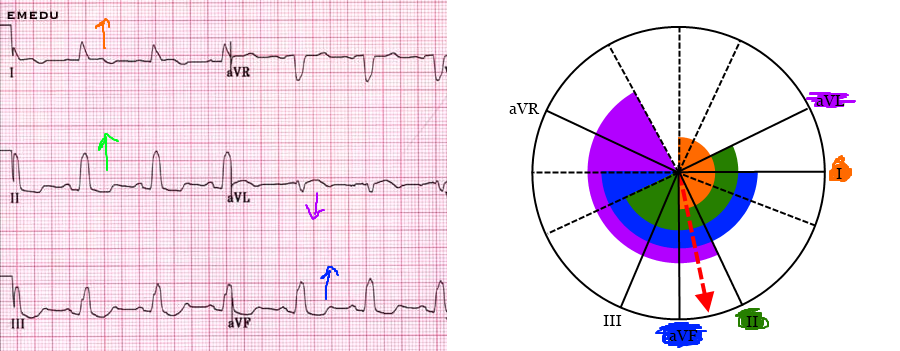
Like this for example
How does one decide where to start on choosing a vector?
Thanks for posting that link Chris. Somehow all this time I have not been aware of you blog. I Love It! Thanks for sharing your excellent knowledge base with us all