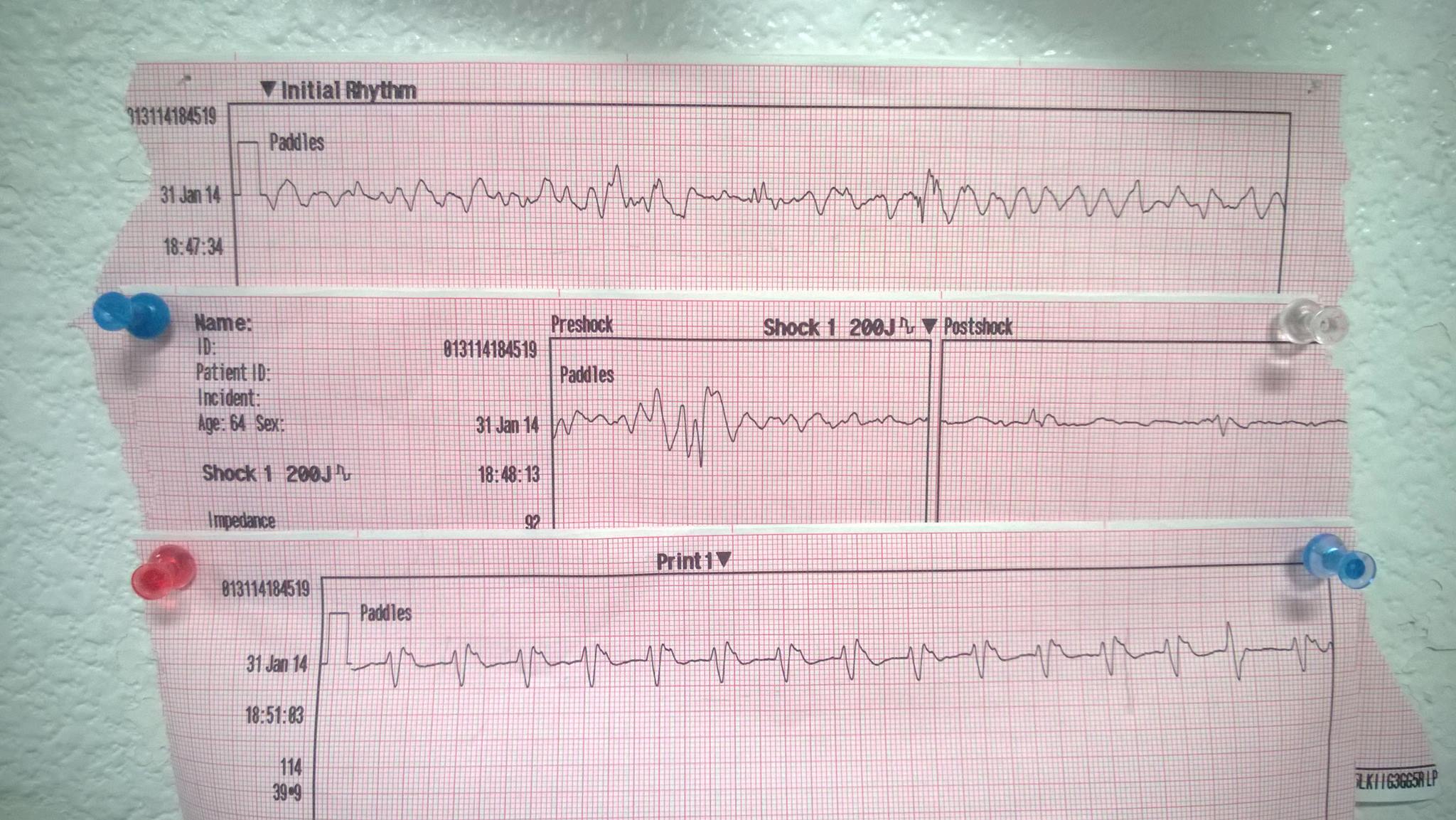
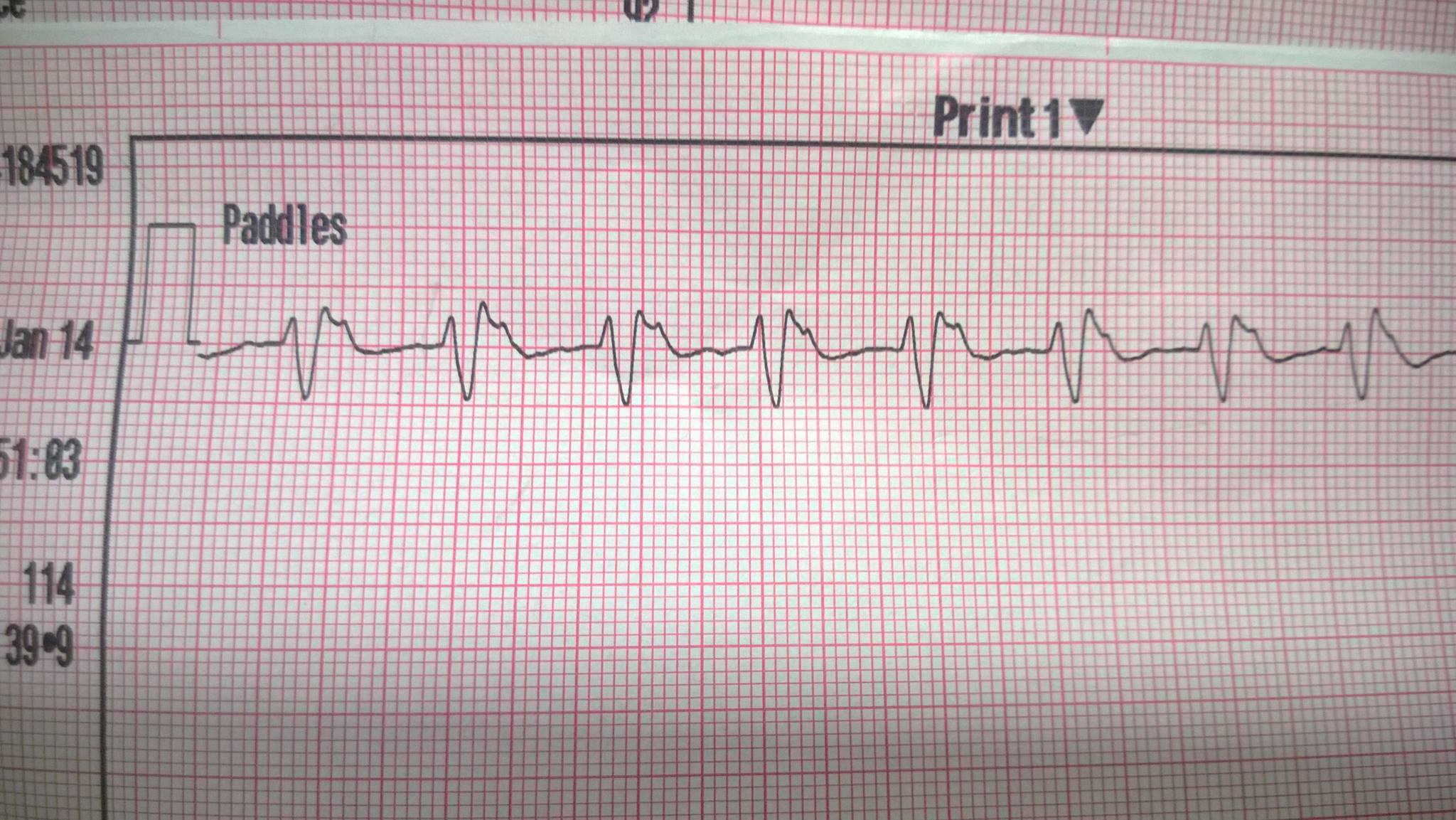
From a full arrest we ran the night before last, slightly less than 10 mins downtime, asystole on scene, to v-fib , shocked, gave more epi, to sinus tach with a pulse. Lost pulse as we were pulling into the ER, they only worked him for ~10 more mins before calling him. He even tried to start breathing on his own again, his thorax was moving like in an agonal respiration.
Edit: Look at that f'ing CO2.
Edit: Look at that f'ing CO2.
