jedirye
Forum Lieutenant
- 114
- 0
- 0
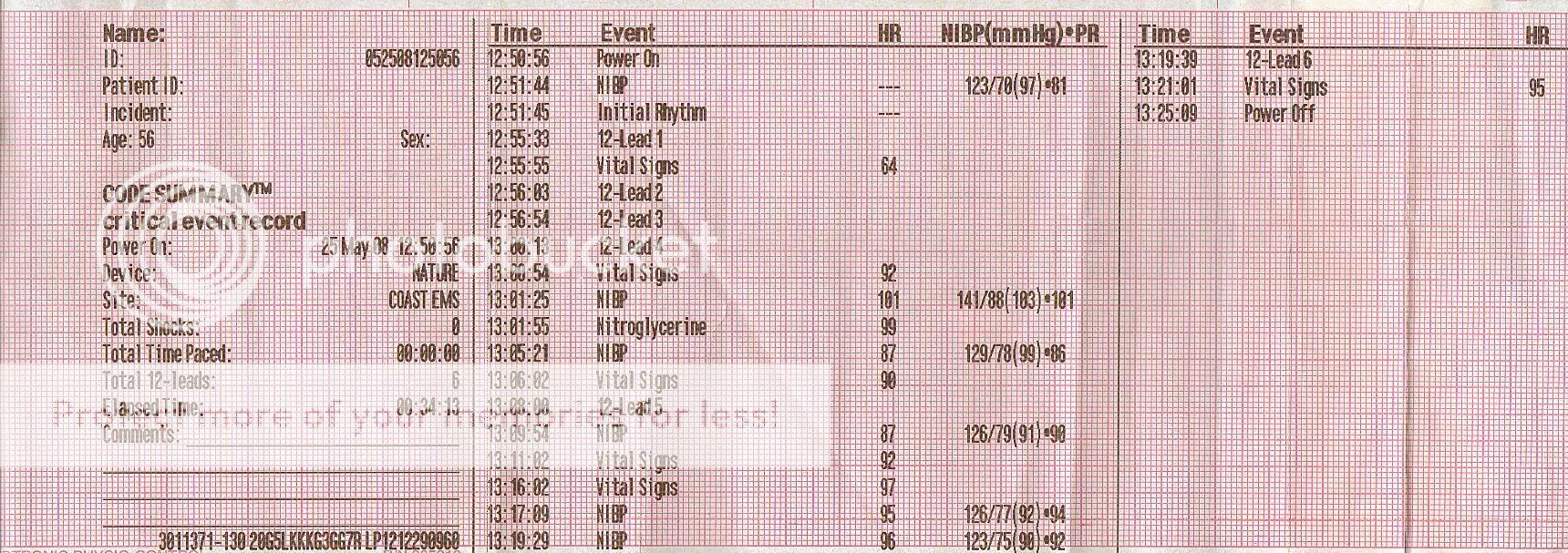
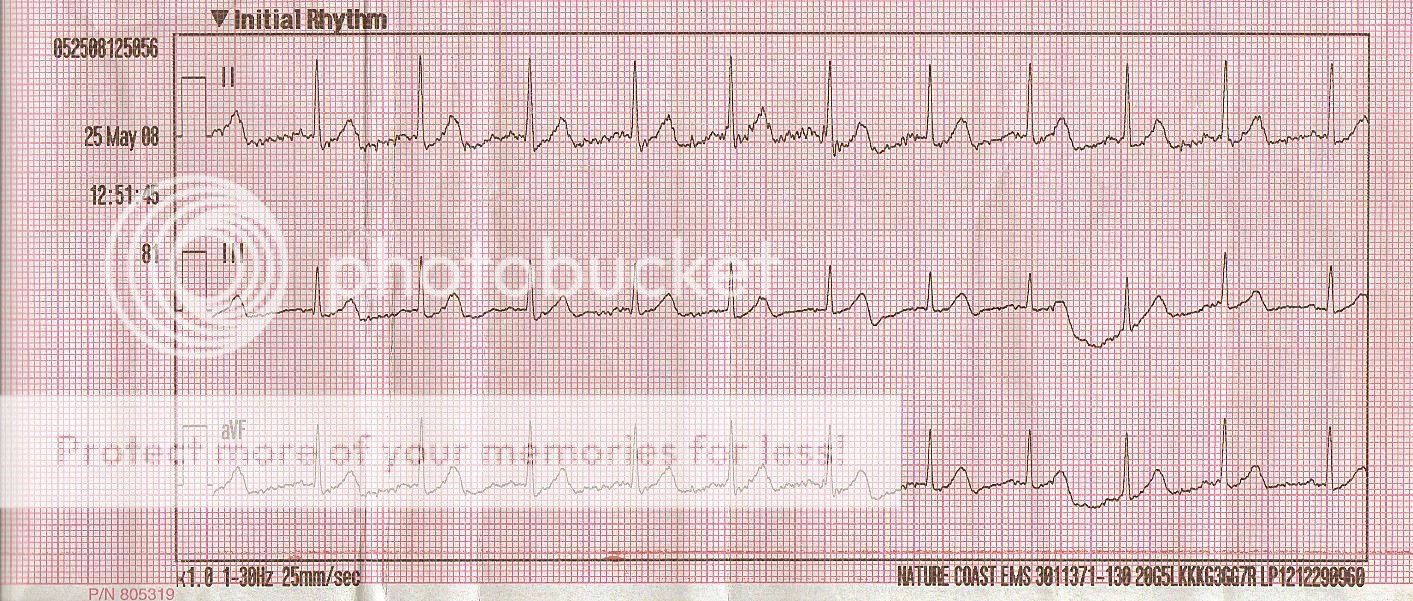
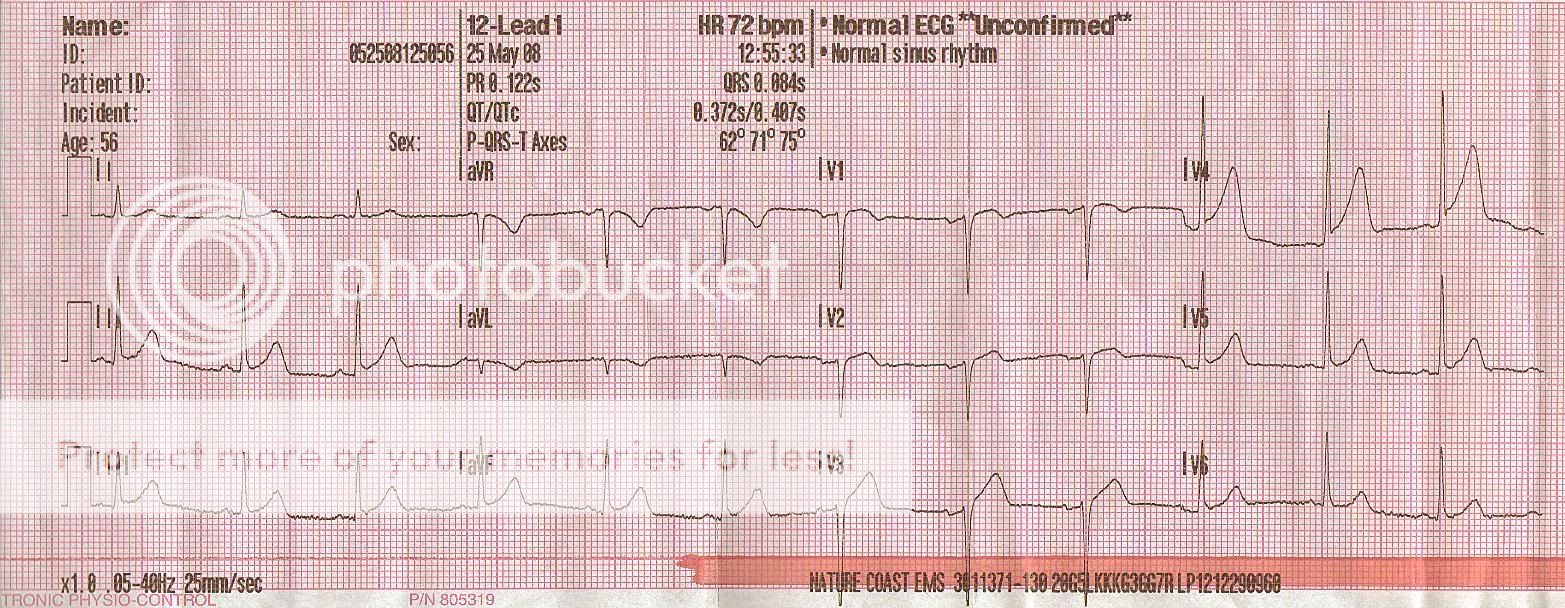
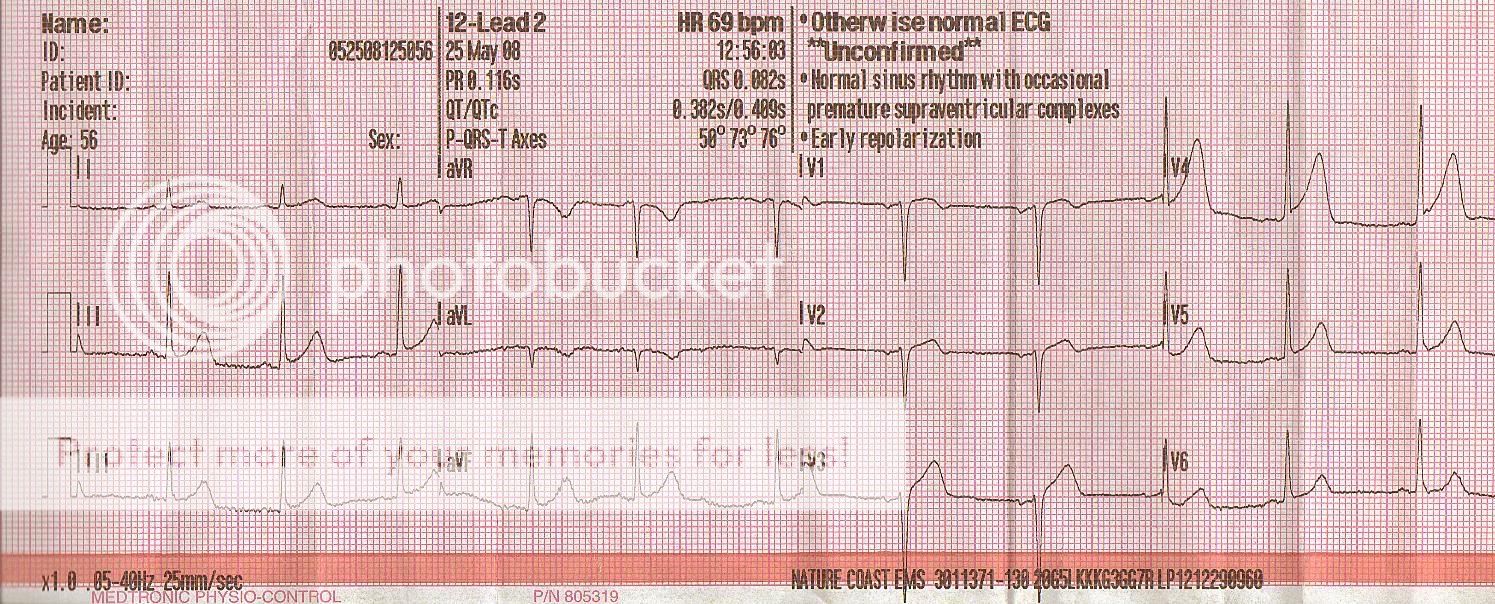
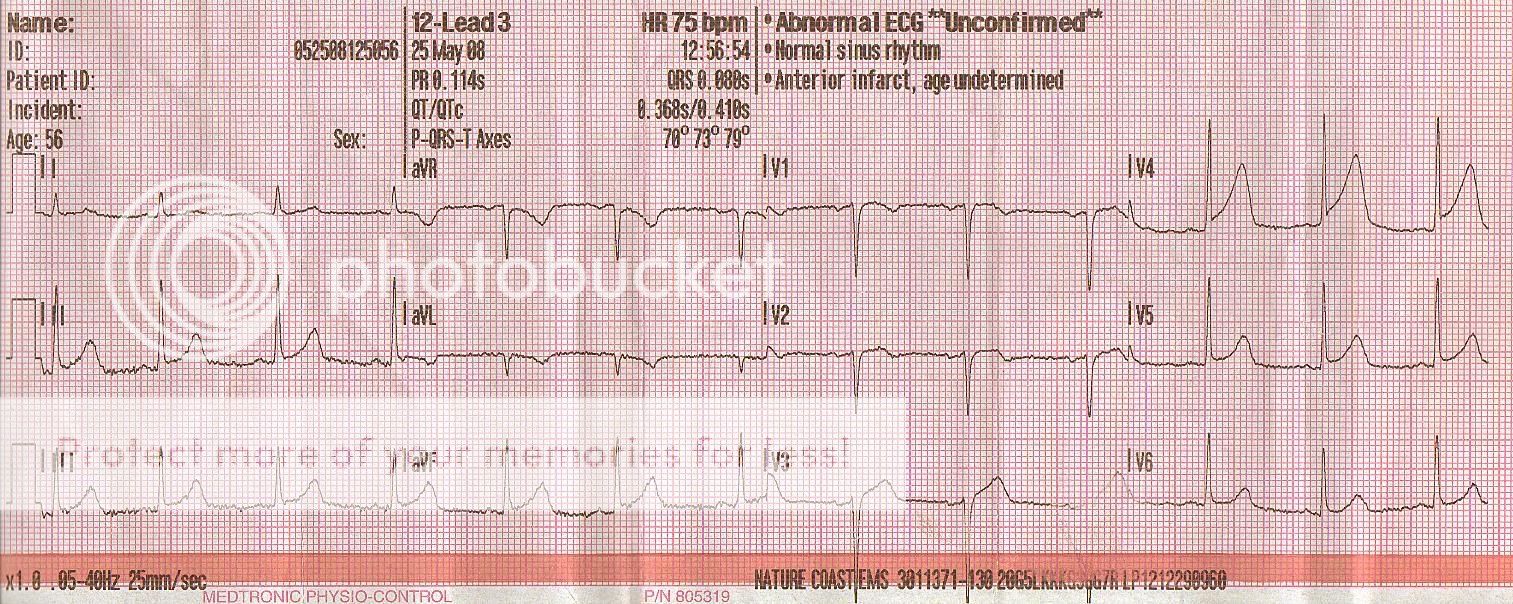
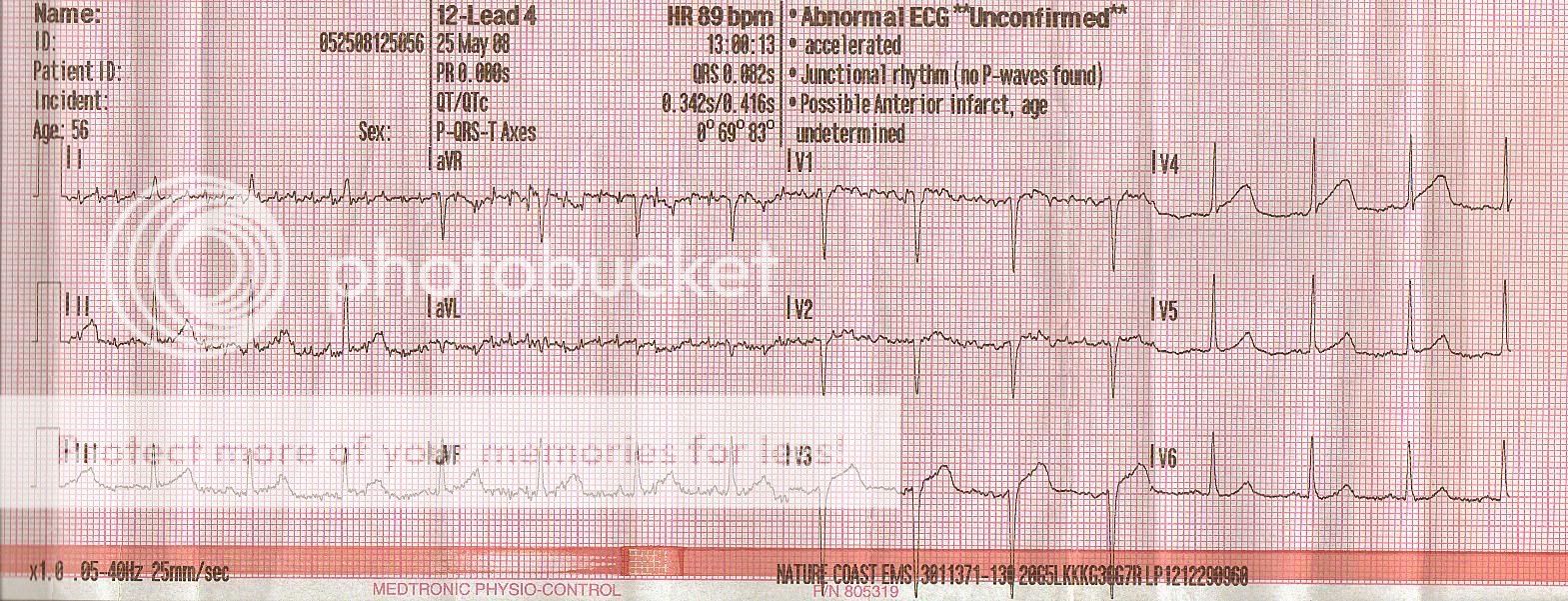
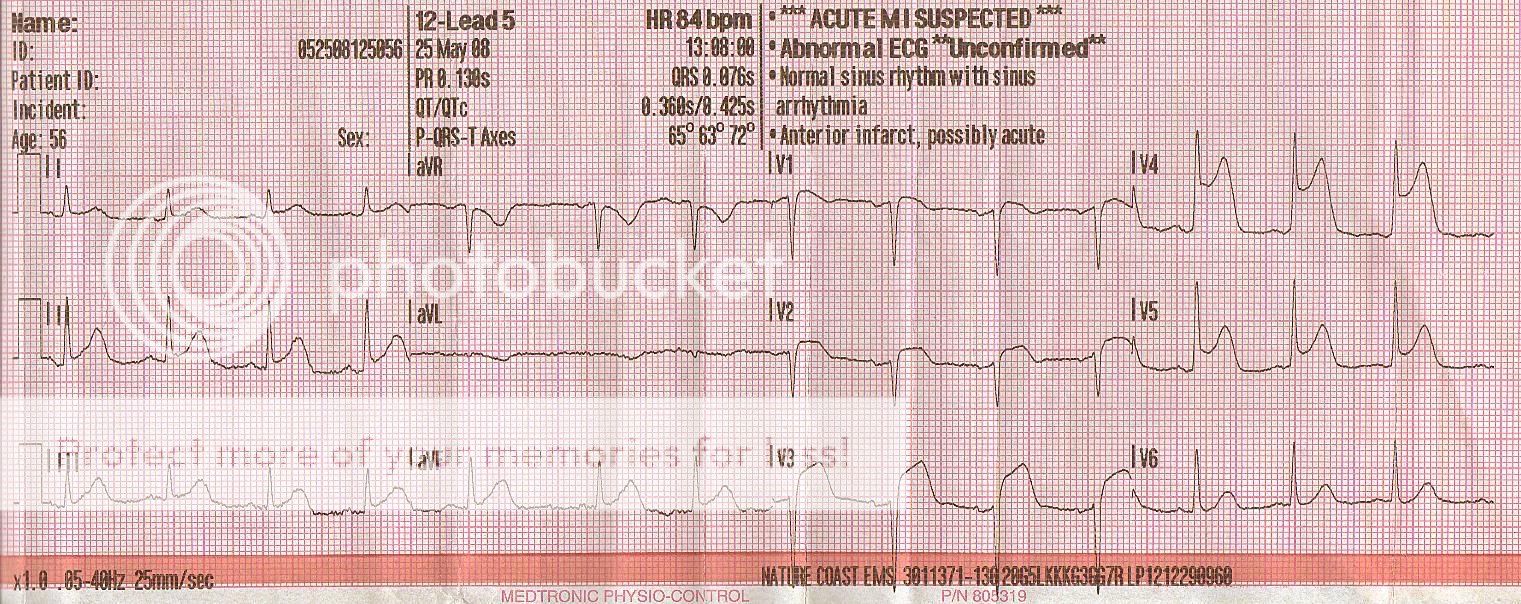
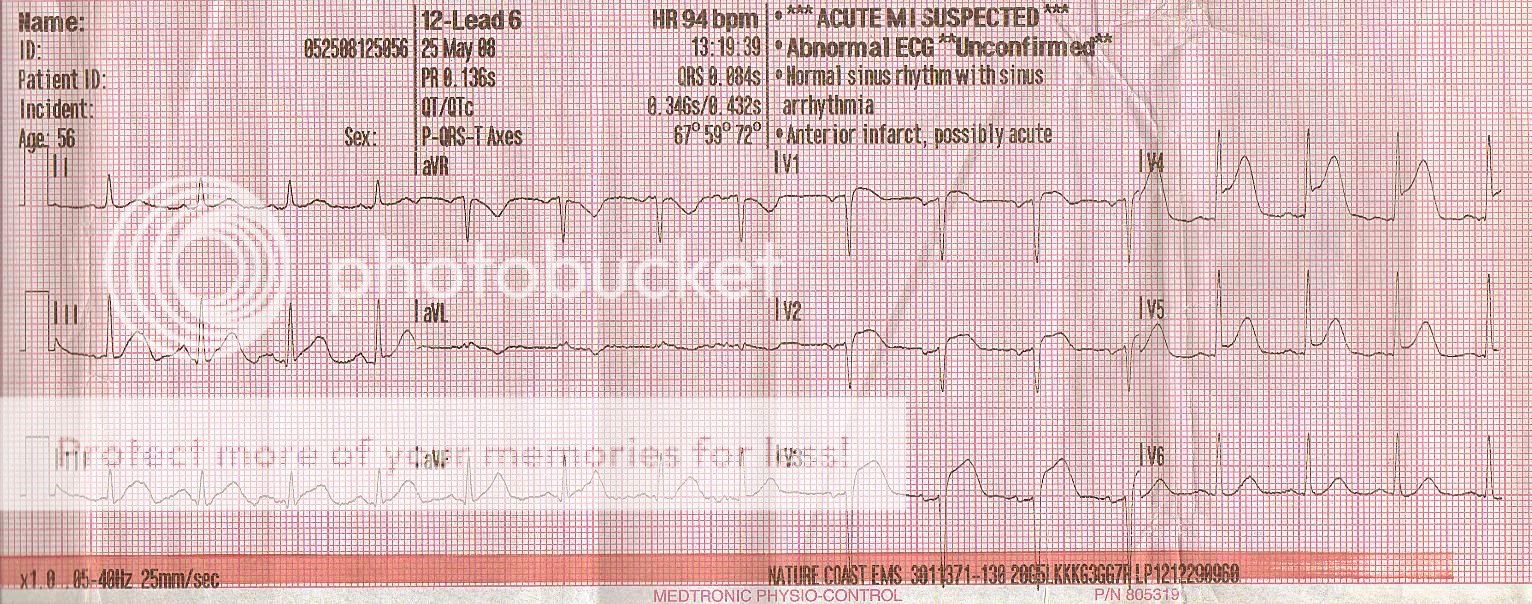
I found this strip while re-reading my EKG book, I guess I was using it as a bookmark or something. I have about 50 other strips scattered about in various locations, I'd like to scan them all but it is terribly time consuming. Figured I would share a cool strip as you can see the progression of ST elevation (hence title). As you can see from the date, it was about a year or so ago so I am not familiar with the story or treatment so take it for what you may. I found it quite interesting to note the time line of the 12-leads and the importance of repeat 12-leads...
-rye
-rye