Tigger
Dodges Pucks
- 7,904
- 2,879
- 113
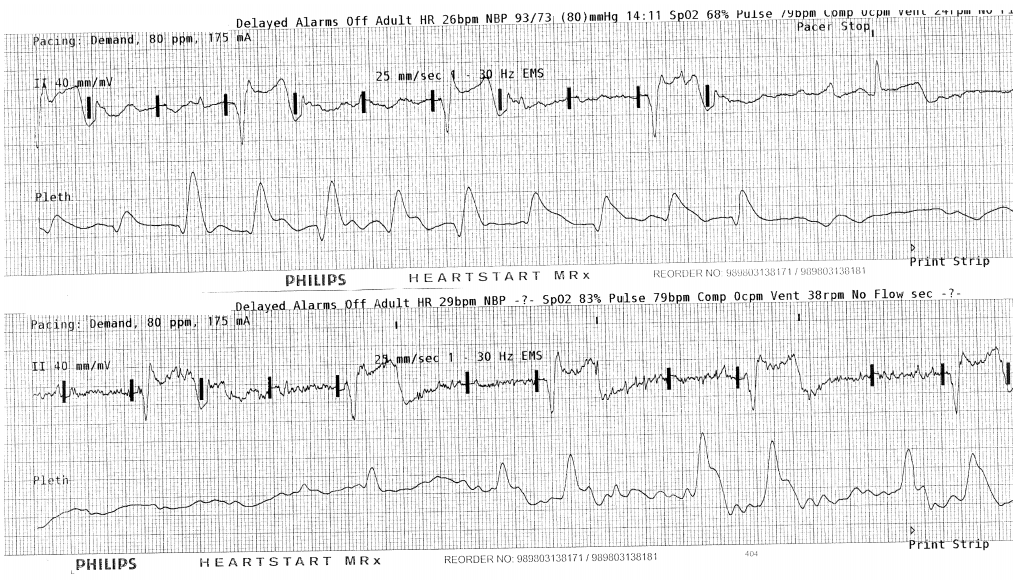
Will find it in a bit, but there’s some research suggesting that folks of all levels are pretty awful at recognizing mechanical capture.You can pace effectively without A/P pad placement and a glance at the pulse ox pleth will indicate capture or not. Those things aside, if there are folks that are not trained well in external pacing, how well trained can they be in treating a full arrest?
Pace when indicated.