reaper
Working Bum
- 2,817
- 75
- 48
I will call the funeral home for him! ")
Follow along with the video below to see how to install our site as a web app on your home screen.
Note: This feature may not be available in some browsers.
This one might be to easy ill heres soomething for a time filler till i find a HARD one 57yr old male sudden onset CP and dyspnea no Hx no old ECG

rvi?this one might be to easy ill heres soomething for a time filler till i find a hard one 57yr old male sudden onset cp and dyspnea no hx no old ecg
rvi?
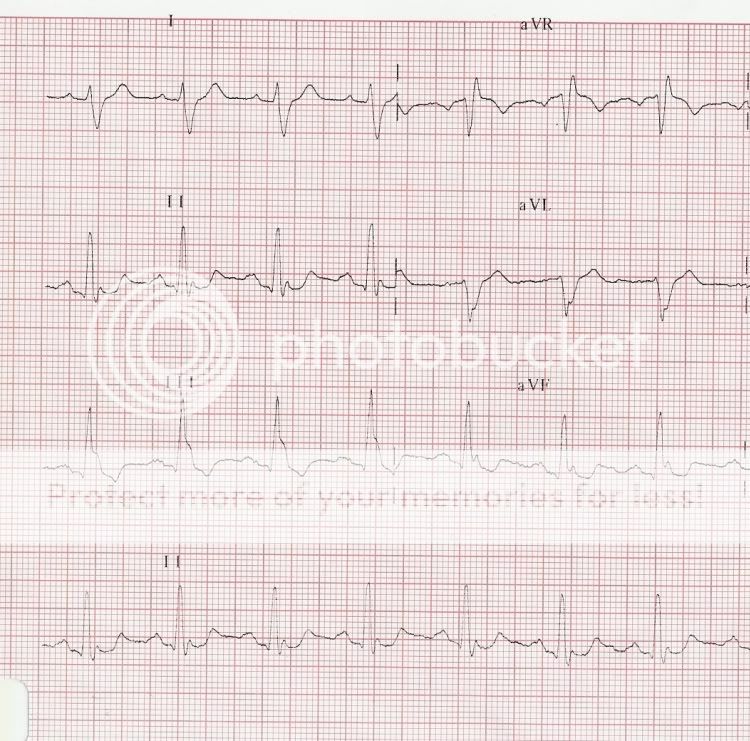
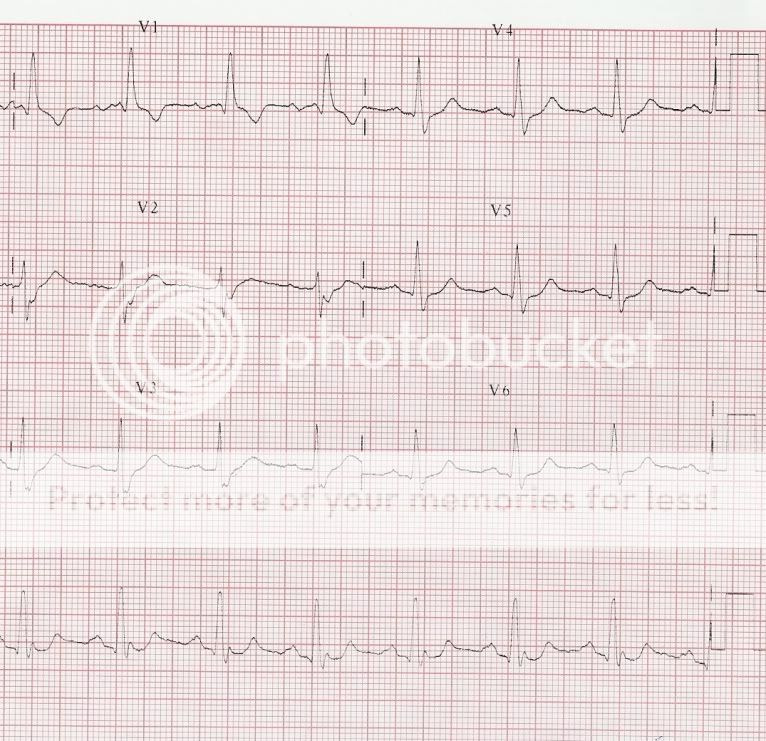
Bifascicular block (RBBB/LPFB-) with borderline 1AVB and left atrial enlargement. Appropriate T-wave discordance. Unusual downward convexity (scooping) of the ST-segment in leads II and aVF and slight ST-elevation in lead aVR. Since the patient has no complaints, this is probably an "old" ECG abnormality.
After QRS 6 am I seeing Winkie Bach?
Do you mean Wenckebach?
And I'm not seeing it.
