firemedic31075
Forum Probie
- 22
- 0
- 0
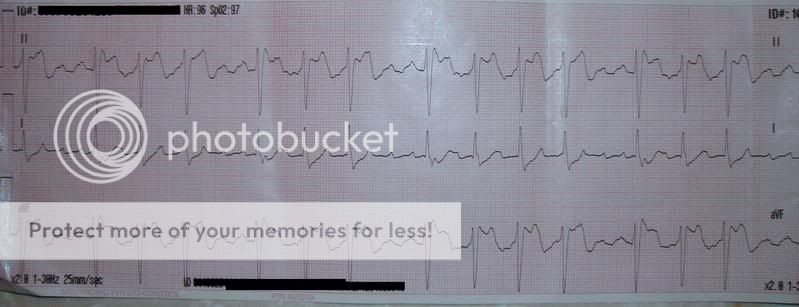
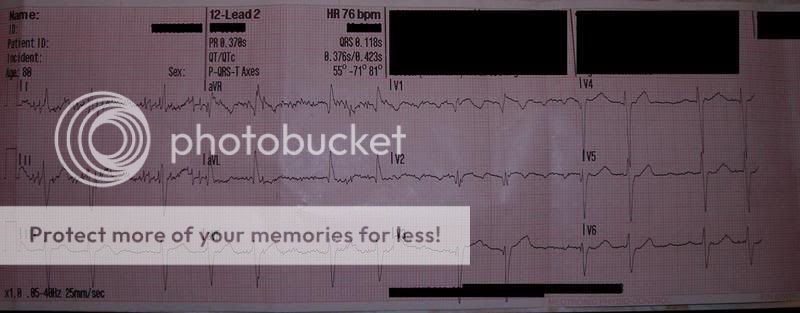
80 y/o/m found at home sitting up in bed. Family says he got into some of his wife's cholesterol medication taking about 9-10 of them 30 mins ago. Daughter states his normal mental status is some what confused but he is a+ox3. patient denies any complaint and says he feels fine. Med Hx- hypertension, A-fib, diabetes. Meds- Insulin, metaprolol etc. VS- b/p- 140/98. P- irregular. R- 18/min. Pupils-PERRL. LS- clear+ equal bilat. Skin- warm and dry. BS- 408 (pt st's he just ate and hasnt taken his insulin tonight). EKG- see below....looks to me like it could be a few different things but was curious what you all thought.