So got thrown for a loop with equipment today. Give me your top guesses without 12 lead since it didn't work til later in the call and I will add it later as it happened for me.
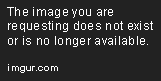
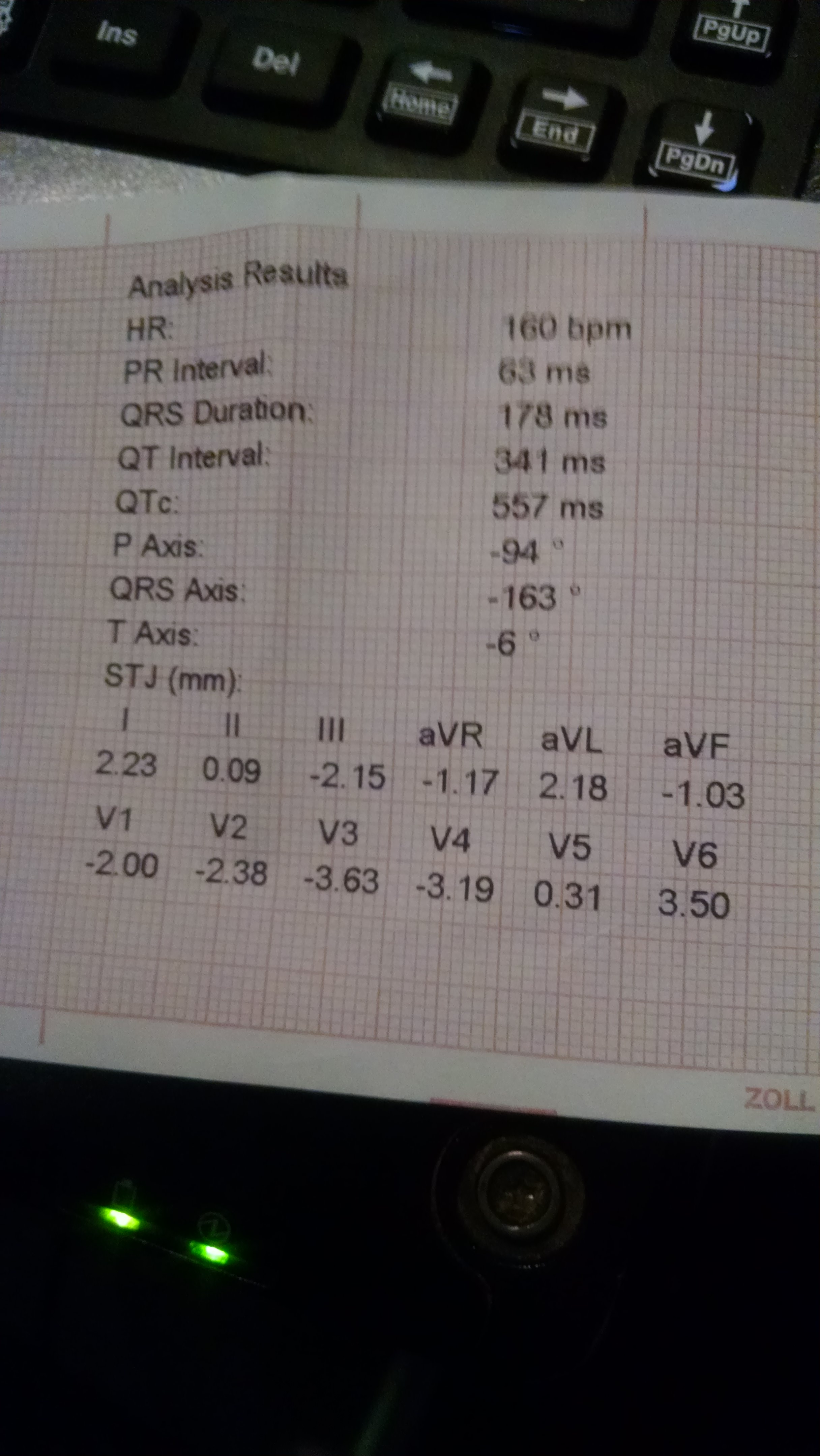
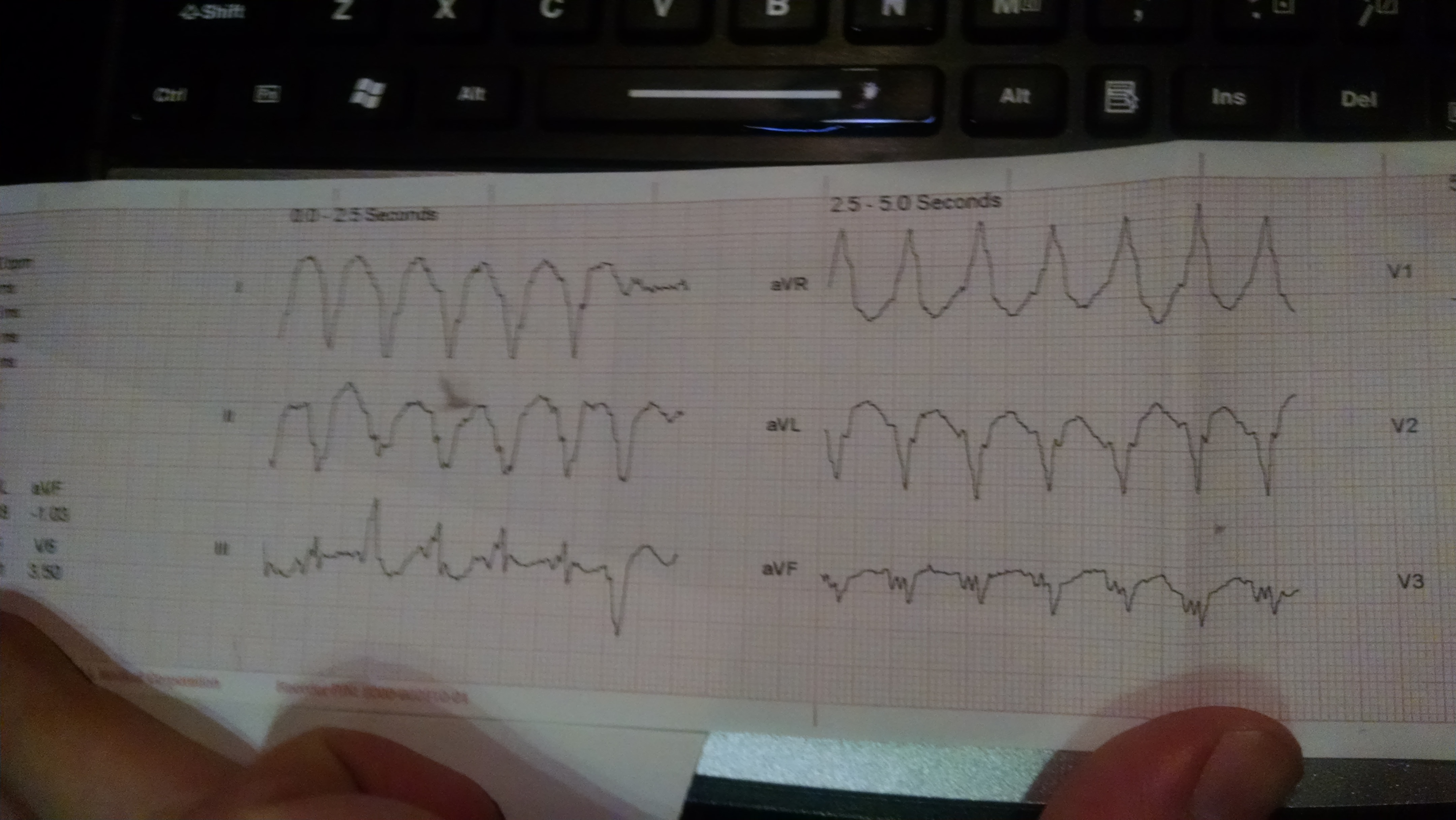
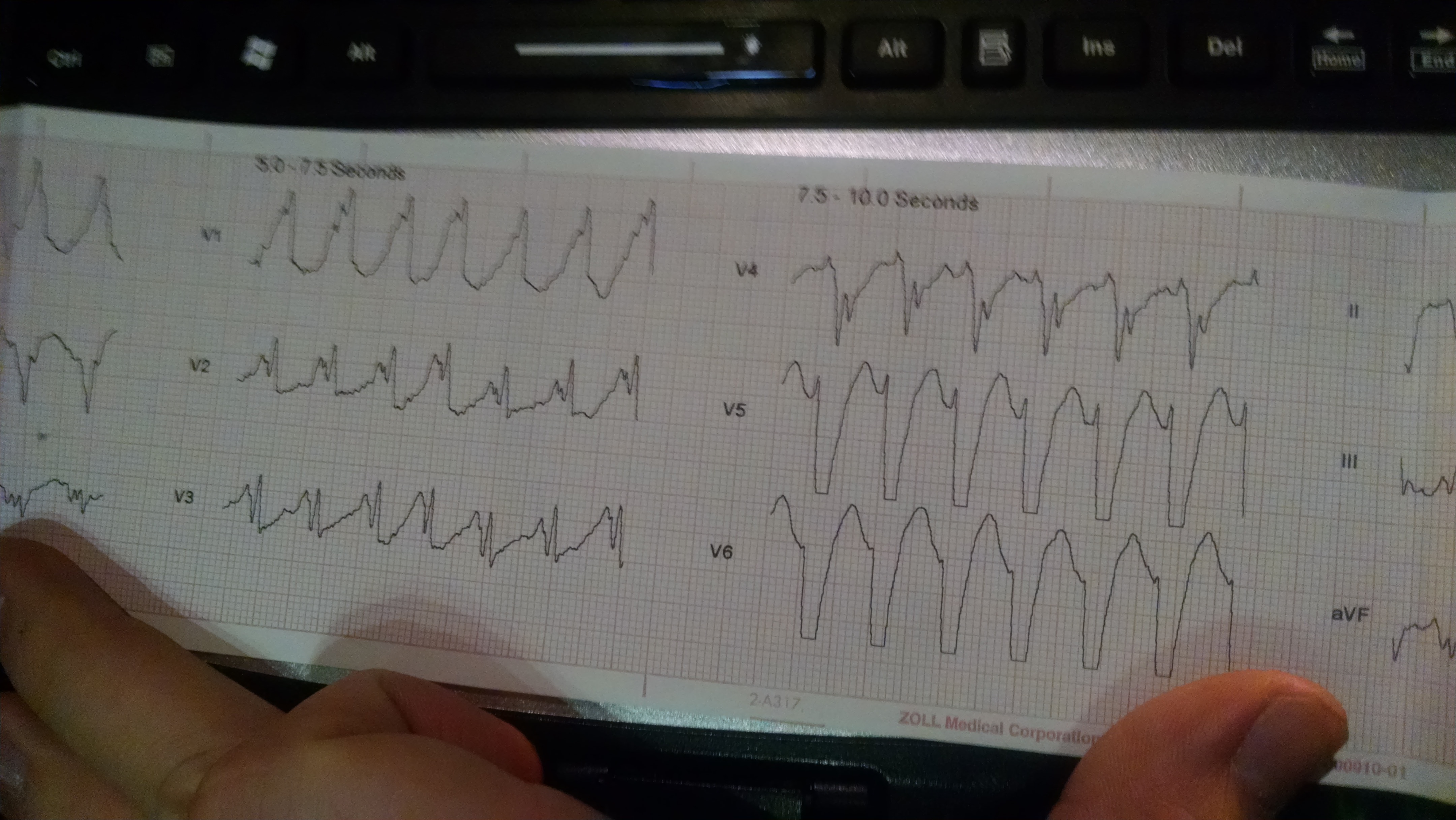
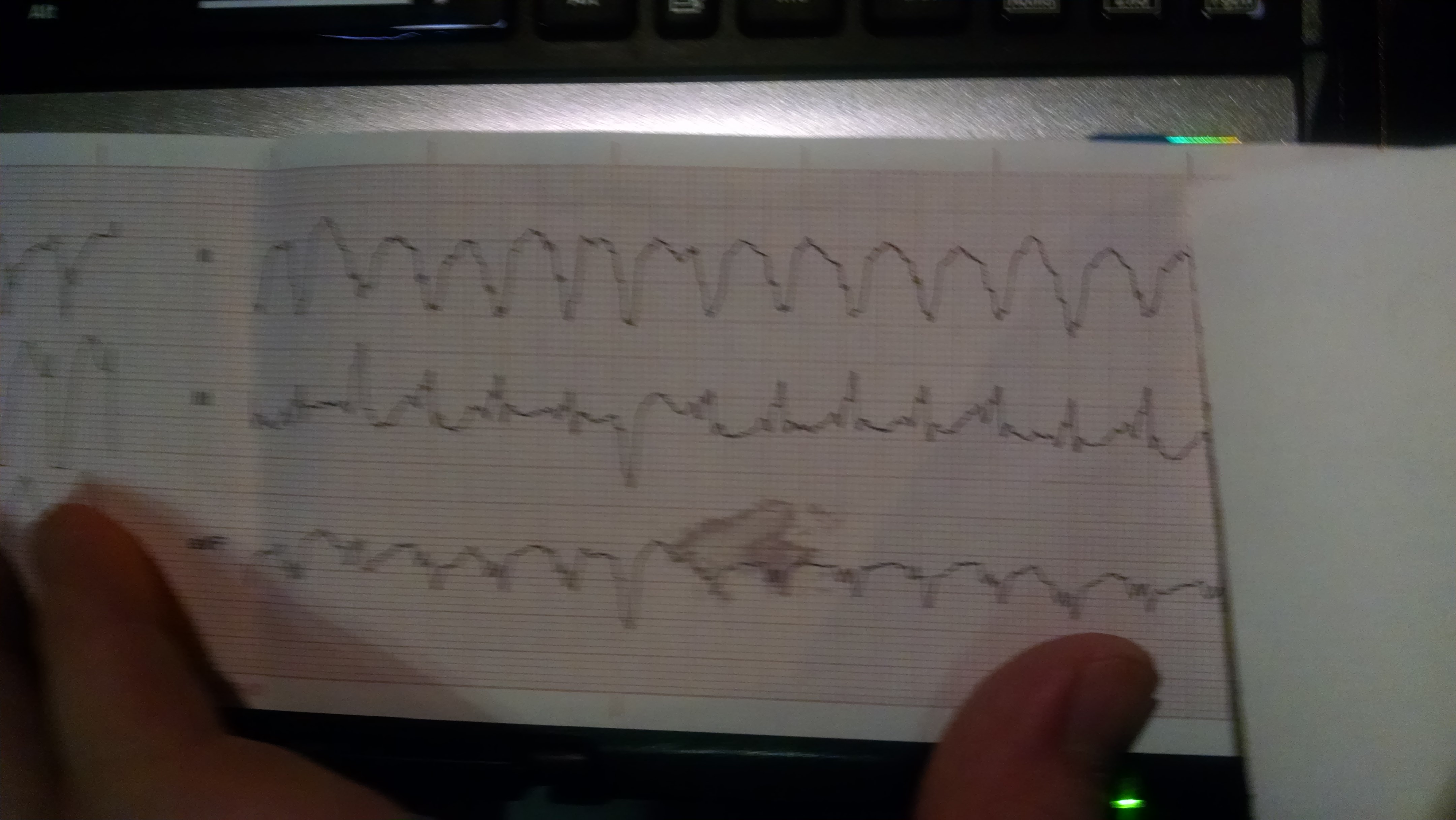
63 y/o m complaining of shortness of breath. Sitting upright, not pale or diaphoretic, good lung sounds in all fields although slightly tachypneic. Says he became short of breath in the shower about 30 minutes ago. He is an immigrant, so clear history is hard to get, but you get that he had a leaky valve. Pulse was weak and rapid, hard to track it well enough to get an exact number, but definitely tachycardic. BP was 120/70's, SpO2 was 78%. Holding nitro and said he took two and they made his breathing feel better, no pedal edema or wet lungs though. 12 lead says lead fault, you gotta check it, so until it works, what are your first few differentials?
63 y/o m complaining of shortness of breath. Sitting upright, not pale or diaphoretic, good lung sounds in all fields although slightly tachypneic. Says he became short of breath in the shower about 30 minutes ago. He is an immigrant, so clear history is hard to get, but you get that he had a leaky valve. Pulse was weak and rapid, hard to track it well enough to get an exact number, but definitely tachycardic. BP was 120/70's, SpO2 was 78%. Holding nitro and said he took two and they made his breathing feel better, no pedal edema or wet lungs though. 12 lead says lead fault, you gotta check it, so until it works, what are your first few differentials?