Just wanted to start off by saying......AWESOME assessment! Do you work on a 9-1-1 ALS rig? The reason I ask is because I don't know of many medics that would be so thorough in their neuro assessment......:beerchug:
I had flashbacks from my Neuroscience class when I read your scenario, I bet
JPINFV and
Veneficus will agree
")
I apologize if this turns out to be a long explanation but I'll try to keep it concise. You were very close to forming a differential diagnosis with Brown-Sequard Syndrome, but there’s a bit more to it than that. Not that I'm a neurosurgeon, but this is my best shot at explaining why your patient presented with the symptoms he did. If you can follow my explanation, I promise you'll have a much better understanding on this "unbalanced PMS" finding.
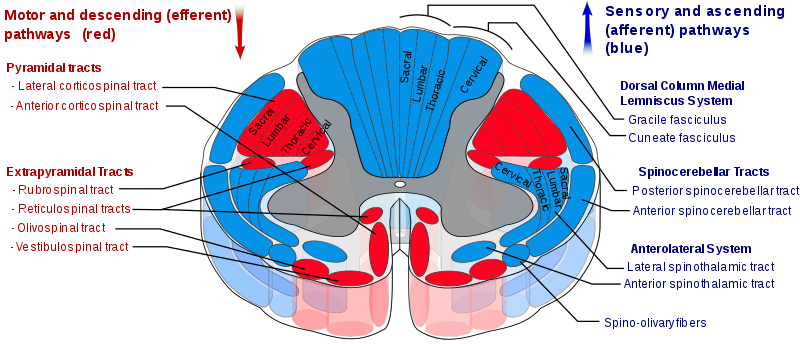
Fine touch and proprioceptive information travel to your brain from the extremities through a pathway in the spinal cord called the "Dorsal Column, Medial Lemniscus System (DC-MLS)" It is located in the posterior-medial part of the spinal cord. Within this system, information at the thoracic level is carried in the "Cuneate fasciculus." This pathway crosses over to the other side of the CNS (i.e. decussate) in the medulla, eventually ending up on the contralateral side of the brain (post-central gyrus).
Using this information, you can localize the lesion on the right side of the spinal cord. I can almost guarantee that if you tested proprioception on your patient’s right hand, it would be as obviously pathologic as your test for fine touch.
But what about the loss of pain in the contralateral arm? Read on…
Pain and crude touch information are transported to the brain through a different pathway called “Spinothalamic Tract (STT)” which is part of the “Anterolateral System.” This system is located in the lateral aspect of the spinal cord. Unlike the DC-MLS, the STT actually decussates in the spinal cord instead of waiting to cross over in the brain stem. The pathway travels up on the contralateral side two vertebral segments above the root and ultimately ends up in the brain very close to the DC-MLS. So, the STT of C5 would be on the contralateral side at C3.
Using this information, it explains why your patient had loss of pain on the left hand but intact fine touch and motor. You stated that the motor was intact in both arms, so the lesion is not close to the corticiospinal tract.
Using all this information, you can localize the lesion around the center of the spinal cord, a bit lateral to the right but medial to the corticospinal tract. This area is supplied the
right lateral branch of the “Anterior Median Spinal Artery” around C4 **C4 because the STT of the left phalanges (C6) will be on the contralateral side at that level**
My best guess is a temporary compression or spasm due to traumatic insult of that blood supply, causing a transient ischemic or inflammatory event. The other parts of both the DC-MLS and STT were spared due to blood supply from the posterior spinal artery.
This is a very localized lesion indeed, but the best one, given the information you provided.
I will encourage critique on this potential diagnosis. It’ll be a learning opportunity for me as well considering this is a REAL case.
I left out quite a bit more detail in an attempt to keep my narrative short for this forum.