NPO
Forum Deputy Chief
- 1,831
- 897
- 113
I'll start off by saying I'm a fairly new paramedic, so this was quite a finding for me, and I thought it was an interesting call. Hopefully someone else will enjoy it.
Responded for an unconcious person. Found a 32 year old male concious on his bed. Reported to have had a syncopal episode and is complaining of SOB for the past day. Room air SPO2 was 66% per the BLS crew on scene who applied a NRB.
HX: mi, Htn, DM, CHF, ESRD, dialysis
Vitals:
Bp: 130/80
Hr: 80
Spo2: 90% on 15lpm
BGL: 30
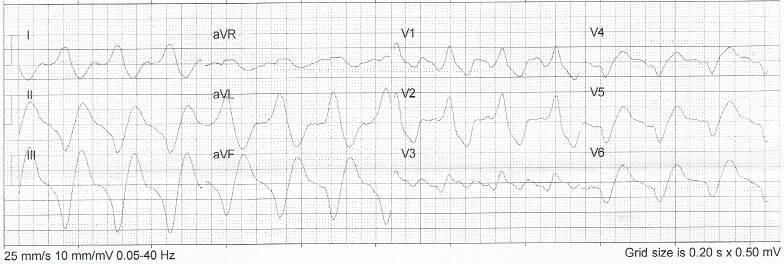
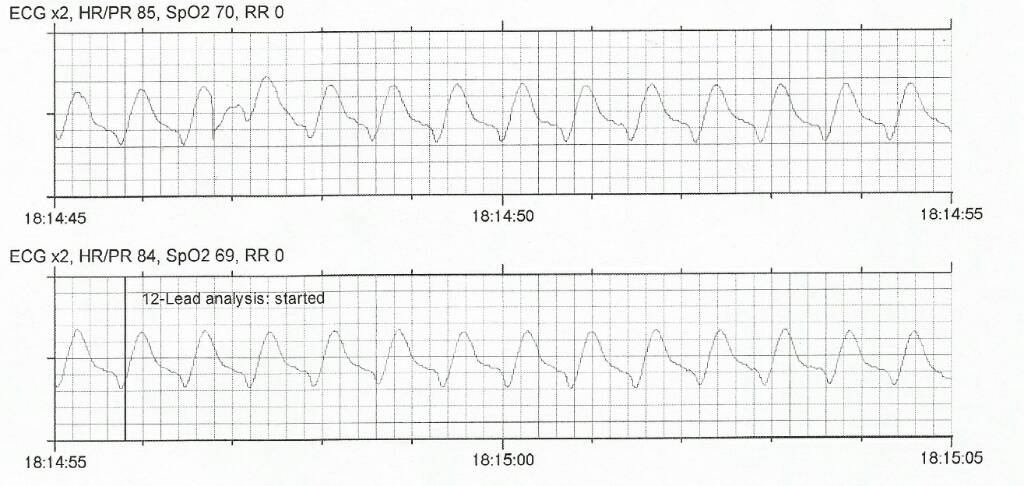
Upon placing the patient on the monitor I noticed the rhythm below. I sent a 12-lead to the hospital. EKG indicated AMI, but I consulted online medical control and told them I believed it to be hyperkalemia, and they concured. They have orders for Bicarb. I never got a line, so I couldn't give meds, but I gave oral glucose. The hospital gave insulin, d50 albuterol, bicarb and calcium gluconate. We all watched him convert to sinus tach.
It was a good call, even though I didn't end up doing much.
Sent from my SM-G935T using Tapatalk
Responded for an unconcious person. Found a 32 year old male concious on his bed. Reported to have had a syncopal episode and is complaining of SOB for the past day. Room air SPO2 was 66% per the BLS crew on scene who applied a NRB.
HX: mi, Htn, DM, CHF, ESRD, dialysis
Vitals:
Bp: 130/80
Hr: 80
Spo2: 90% on 15lpm
BGL: 30
Upon placing the patient on the monitor I noticed the rhythm below. I sent a 12-lead to the hospital. EKG indicated AMI, but I consulted online medical control and told them I believed it to be hyperkalemia, and they concured. They have orders for Bicarb. I never got a line, so I couldn't give meds, but I gave oral glucose. The hospital gave insulin, d50 albuterol, bicarb and calcium gluconate. We all watched him convert to sinus tach.
It was a good call, even though I didn't end up doing much.
Sent from my SM-G935T using Tapatalk
