Hockey
Quackers
- 1,222
- 6
- 38
I want to hear everything you know about it
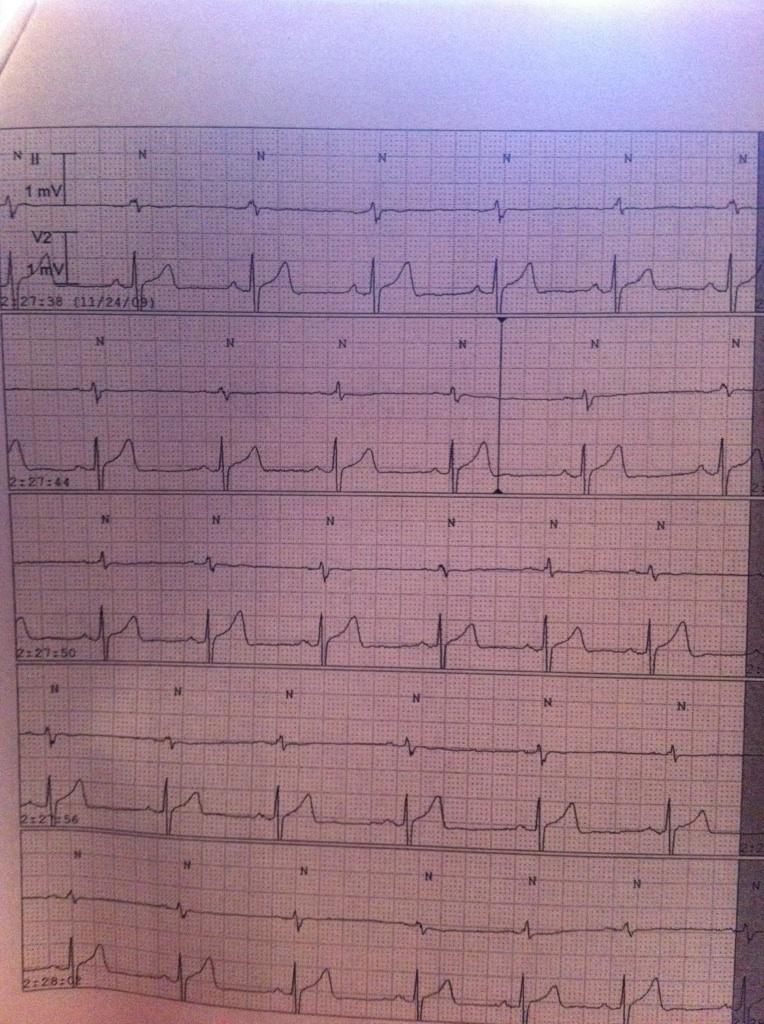
What do we have, any pr qrts r-r qt info
Would like to see what you think
What do we have, any pr qrts r-r qt info
Would like to see what you think
Last edited by a moderator: