Melclin
Forum Deputy Chief
- 1,796
- 4
- 0
I've been wanting to post scenarios regularly even if they aren't noodle scratchers. Just everyday common conundrums so people can compare notes and students/newbies can have a crack without fear of retribution. This is one of those scenarios.
Called to a 28YOM Unconscious/fainting - conscious/breathing/no bleeding.
Approx 15 minute response time.
O/A- You are lead by a calm looking woman in her late 20's to a young bloke lying L lateral, covered with a blanket, in a reasonably cramped corridor on a cold wooden floor.
He is conscious and talking to you. Him and his wife were having an argument when she observed him to drop to the floor followed by 10-20 seconds of upper limb rigidity and looking like he was gasping. She is unsure about any other seizure activity when asked. The pt then experienced approx 5 mins of drowsiness and confusion per the wife and but the pt contests that saying he just felt really tired but does not remember the shaking limbs or falling to the ground. Asymptomatic after 5 mins.
O/E BP: 110/60. HR 80. RR 16. Temp: 36.5 (97.7). BSL: 4.9 (90). SpO2 98% GCS 15.
HEENT/Neuro: PEARL, Normal eye exam (movement/acuity). Normal mental status per wife, alert, maybe a little sombre. Nil head/neck pain/c-spine pain on palpation. Normal movement of facial muscles, normal speech. Head/neck is atraumatic.
Trunk: Chest is clear and equal. Equal exansion, no distress/accessory muscles evident. Heart sounds normal. Nil, chest pain/abdo pain, palpitations, SOB or nausea. Abdomen is soft and atraumatic.
Limbs/Extremities: Hands are cold and reasonably pale. Equal/normal strength/sensation in limbs.
Medical Hx.
-When asked, pt has a hx 8 months previous of syncope after a bowel motion while he had gastro, investigated in the ED. Had and ECG done at the time and they though he may have had a heart attack. He knows nothing more about this.
-Asthma, well controlled, infrequently uses puffer.
Generally fit and well of late. Normal bowel motions/micturition.
Meds
Albuterol
Allergies
Penicillin
Social hx
Nil drugs, drink infrequently. Works as a electrician. Is currently at the house you've been called to visiting relatives for the weekend. They've had a nice time and the argument with the wife was about whether or not they could afford to stay another few days.
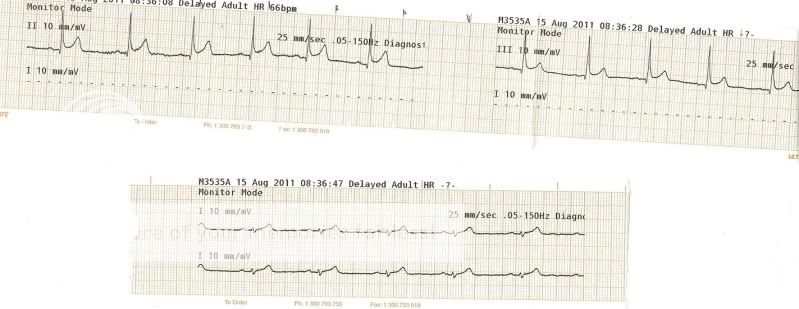
ECG shows ST elevation in leads II and III. I'll post the strip in a few hours when my printer starts working.
Called to a 28YOM Unconscious/fainting - conscious/breathing/no bleeding.
Approx 15 minute response time.
O/A- You are lead by a calm looking woman in her late 20's to a young bloke lying L lateral, covered with a blanket, in a reasonably cramped corridor on a cold wooden floor.
He is conscious and talking to you. Him and his wife were having an argument when she observed him to drop to the floor followed by 10-20 seconds of upper limb rigidity and looking like he was gasping. She is unsure about any other seizure activity when asked. The pt then experienced approx 5 mins of drowsiness and confusion per the wife and but the pt contests that saying he just felt really tired but does not remember the shaking limbs or falling to the ground. Asymptomatic after 5 mins.
O/E BP: 110/60. HR 80. RR 16. Temp: 36.5 (97.7). BSL: 4.9 (90). SpO2 98% GCS 15.
HEENT/Neuro: PEARL, Normal eye exam (movement/acuity). Normal mental status per wife, alert, maybe a little sombre. Nil head/neck pain/c-spine pain on palpation. Normal movement of facial muscles, normal speech. Head/neck is atraumatic.
Trunk: Chest is clear and equal. Equal exansion, no distress/accessory muscles evident. Heart sounds normal. Nil, chest pain/abdo pain, palpitations, SOB or nausea. Abdomen is soft and atraumatic.
Limbs/Extremities: Hands are cold and reasonably pale. Equal/normal strength/sensation in limbs.
Medical Hx.
-When asked, pt has a hx 8 months previous of syncope after a bowel motion while he had gastro, investigated in the ED. Had and ECG done at the time and they though he may have had a heart attack. He knows nothing more about this.
-Asthma, well controlled, infrequently uses puffer.
Generally fit and well of late. Normal bowel motions/micturition.
Meds
Albuterol
Allergies
Penicillin
Social hx
Nil drugs, drink infrequently. Works as a electrician. Is currently at the house you've been called to visiting relatives for the weekend. They've had a nice time and the argument with the wife was about whether or not they could afford to stay another few days.
ECG shows ST elevation in leads II and III. I'll post the strip in a few hours when my printer starts working.