Austin carawan
Forum Crew Member
- 52
- 4
- 8
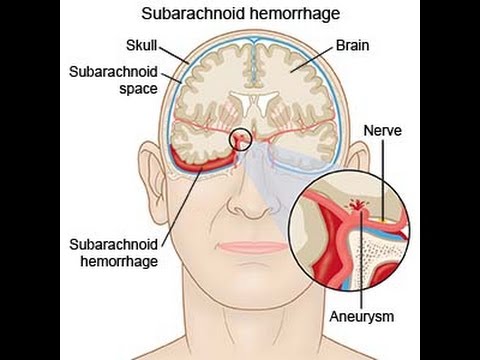
ive narrowed it down to these two, the patient has the worst headache of her life, with rapid onset, and blurred vision, and her left arm is weak,(tell tail stroke sign right?) she feels nauseous and her speech is slurred,are there any findings in stroke not seen in an aneurysm l, and vice versa, either way transport is indicated. But with mainly book experience on these two they appear similar in their symptoms