korvus
Forum Ride Along
- 9
- 0
- 0
I saw this ECG from a patient the other day who complained of 7/10 chest pain originally, but claimed he was down to 1-1.5/10 by the time we arrived. He only went in the ambulance because his wife insisted.
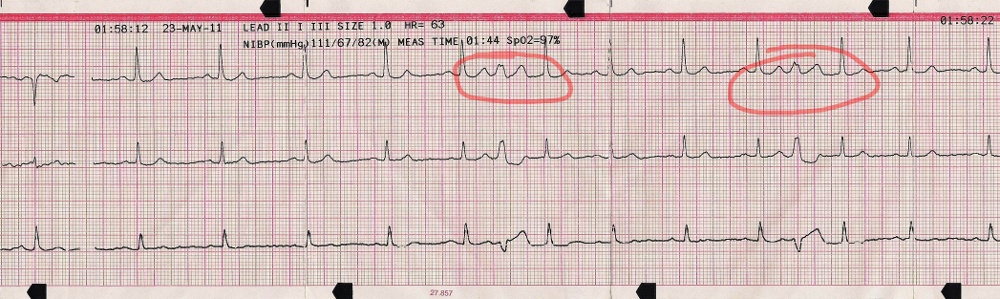
It looks to me like perhaps non-conducting PACs? Perhaps one-ventricular-beat-wide runs of A-flutter? I find it odd mostly because these always showed up right between the T and P waves, which made me think the ventricular activity had something to do with it (not just something odd going on in the atria). Based on the morphology across the leads, it's obvious something different is going on for that middle bump versus normal P/T waves.
I'll note the patient could feel when these happened. I guess my best analysis would be PACs and the atria only fired at those times because any other time, whenever they tried to fire, they were in a refractory state. But I'd love to hear what others have to say.
I'd also be interested in what this means for the patient. We'd see 2-3 of these, separated by a few normal beats, every minute or two. So they were frequent, but he seemed hemodynamically stable...
Thanks!
It looks to me like perhaps non-conducting PACs? Perhaps one-ventricular-beat-wide runs of A-flutter? I find it odd mostly because these always showed up right between the T and P waves, which made me think the ventricular activity had something to do with it (not just something odd going on in the atria). Based on the morphology across the leads, it's obvious something different is going on for that middle bump versus normal P/T waves.
I'll note the patient could feel when these happened. I guess my best analysis would be PACs and the atria only fired at those times because any other time, whenever they tried to fire, they were in a refractory state. But I'd love to hear what others have to say.
I'd also be interested in what this means for the patient. We'd see 2-3 of these, separated by a few normal beats, every minute or two. So they were frequent, but he seemed hemodynamically stable...
Thanks!