Hey, so this was a tricky one for me so figured would be good to post it here and get some more feedback!
50yo M, A&0X4. Sitting in chair complaining of difficulty breathing that was exaccerbated by going out to his garage with physical exertion. History of asthma and hypertension. He's satting 88% RA, Skins are Very diaphoretic but its also 110 degree's outside at the time. He's in moderate resp distress at about 25 resp and slightly labored.
No chest pain, nausea, vomiting, weakness, dizziness, confusion, syncope or any other complaints. He denies any cardiac history whatsoever aside from asthma and hypertension (i SUPPOSE you could say thats cardiac? but splitting hairs in a way......i digress)
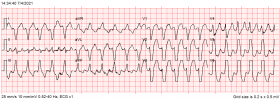
Get him on monitor and 4 lead is showing a sorta bigeminy ranging between 130's to 200's and just all over the place. Im thinking AFIB RVR new onset possibly. We get out to the rig and 12 lead Is Left bundle branch block but tachy as **** still ranging between 130's to 200's.......200's isnt sustained and only briefly stays there and he's more on the lower end. Lungs are pretty clear, VERY minimal wheezing so i do a duoneb just to rule it out. Get IV enroute.
The duoneb actually somewhat improved his resp status with SP02 now at 95%, resp rate to about 20 and minimally to not labored anymore.
BP 150's systolic (hypertension history)
We go Code 3 to hospital and transport time is less than 3 minutes. Hospital almost immediately hits him with adenosine...... No change.
I left after that but they were talking about cardioversion.
I hesitated a bit because how am i gonna Adenosine someone with a Wide complex rhythm that appears left bundle branch block? Lidocain is in our protocols for a wide complex but again....With his rate jumping all over the place im thinking there's an underlying rhythm such as Afib rvr Or something else that i cant see?
What would you guys have done differently?
(ps i'll try to attach the 12 lead soon. but its basically just a left bundle branch block at a rate of 131bpm)
50yo M, A&0X4. Sitting in chair complaining of difficulty breathing that was exaccerbated by going out to his garage with physical exertion. History of asthma and hypertension. He's satting 88% RA, Skins are Very diaphoretic but its also 110 degree's outside at the time. He's in moderate resp distress at about 25 resp and slightly labored.
No chest pain, nausea, vomiting, weakness, dizziness, confusion, syncope or any other complaints. He denies any cardiac history whatsoever aside from asthma and hypertension (i SUPPOSE you could say thats cardiac? but splitting hairs in a way......i digress)
Get him on monitor and 4 lead is showing a sorta bigeminy ranging between 130's to 200's and just all over the place. Im thinking AFIB RVR new onset possibly. We get out to the rig and 12 lead Is Left bundle branch block but tachy as **** still ranging between 130's to 200's.......200's isnt sustained and only briefly stays there and he's more on the lower end. Lungs are pretty clear, VERY minimal wheezing so i do a duoneb just to rule it out. Get IV enroute.
The duoneb actually somewhat improved his resp status with SP02 now at 95%, resp rate to about 20 and minimally to not labored anymore.
BP 150's systolic (hypertension history)
We go Code 3 to hospital and transport time is less than 3 minutes. Hospital almost immediately hits him with adenosine...... No change.
I left after that but they were talking about cardioversion.
I hesitated a bit because how am i gonna Adenosine someone with a Wide complex rhythm that appears left bundle branch block? Lidocain is in our protocols for a wide complex but again....With his rate jumping all over the place im thinking there's an underlying rhythm such as Afib rvr Or something else that i cant see?
What would you guys have done differently?
(ps i'll try to attach the 12 lead soon. but its basically just a left bundle branch block at a rate of 131bpm)