You are using an out of date browser. It may not display this or other websites correctly.
You should upgrade or use an alternative browser.
You should upgrade or use an alternative browser.
EKG Interps Part 2
- Thread starter tah06090
- Start date
the_negro_puppy
Forum Asst. Chief
- 897
- 0
- 0
WOw interesting ECG, i'll have a stab, cant guarantee ill be right!
Rate, around 120?
Rhythm? Sinus tach?
Ischaemia: S-T elevation in leads II, and aVF
S-t Depression in I, aVL,
Wide complexes perhaps a LBBB?
Soz if im abit out, still consolidating 12 lead ECGs, plus jsut got home from 12 hour night shift")
Rate, around 120?
Rhythm? Sinus tach?
Ischaemia: S-T elevation in leads II, and aVF
S-t Depression in I, aVL,
Wide complexes perhaps a LBBB?
Soz if im abit out, still consolidating 12 lead ECGs, plus jsut got home from 12 hour night shift
MSDeltaFlt
RRT/NRP
- 1,422
- 35
- 48
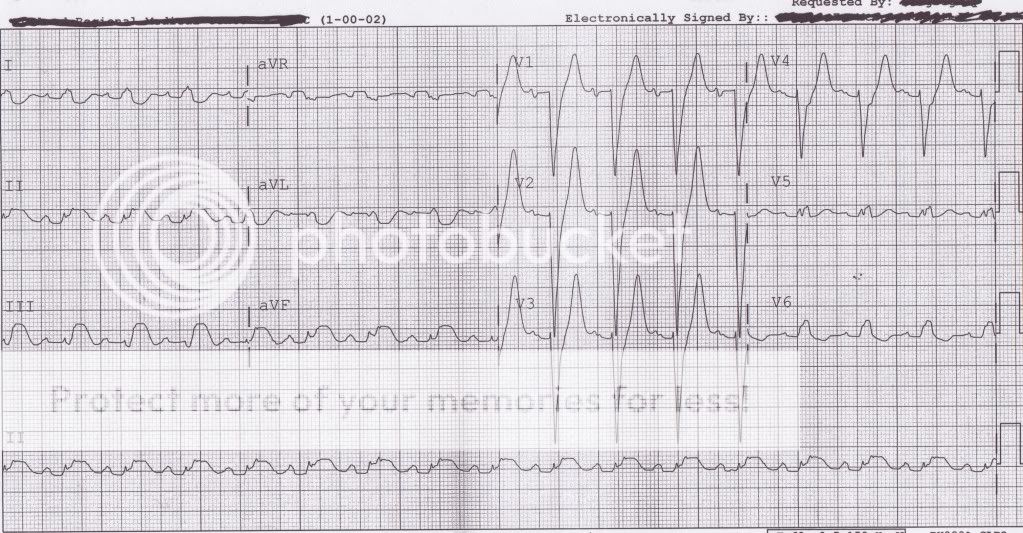
HR = 94. SR /c LBBB 1°AVB. Not to mention the inferior MI effecting the RCA.
ekgpress
Forum Probie
- 18
- 0
- 0
EKG Interprs Part 2 ALS Discussion
Sinus rhythm - LBBB - acute inferior STEMI (with primary ST elevation in inferior leads). Reciprocal ST depression in aVL, if not I, V4. This is one for the cath lab - Ken -
72 yr old male presents to ED with SOB for 5 hrs here ya go
Sinus rhythm - LBBB - acute inferior STEMI (with primary ST elevation in inferior leads). Reciprocal ST depression in aVL, if not I, V4. This is one for the cath lab - Ken -
72 yr old male presents to ED with SOB for 5 hrs here ya go
TomB
Forum Captain
- 393
- 82
- 28
Meets Sgarbossa's criteria with concordant ST-elevation in the inferior leads and ST-depression in the right precordial leads but I would like to know more about the history and clinical presentation as hyperkalemia is one of the "great imitators".
celticcare
Forum Ride Along
- 3
- 0
- 1
looking at it, definatly the ST Elevation inferirorly, reciprical ST depression, but the very peaked t's are making me wonder if there is a septal lead Pacemaker or even localised pericarditis issues. Normal axis so aren't thinking cor pulmonalae or anything like that.
looking at it, definatly the ST Elevation inferirorly, reciprical ST depression, but the very peaked t's are making me wonder if there is a septal lead Pacemaker or even localised pericarditis issues. Normal axis so aren't thinking cor pulmonalae or anything like that.
Brown thinks the peaked T waves and deep QR patterns in V1-V4 are perhaps hypertrophy?
mikie
Forum Lurker
- 1,071
- 1
- 36
question...
Are the biphasic P waves in V1 (and perhaps V2) significant of anything?
Are the biphasic P waves in V1 (and perhaps V2) significant of anything?
TomB
Forum Captain
- 393
- 82
- 28
Yes. Left atrial enlargement which implies LVH (as does the LBBB).
Are the biphasic P waves in V1 (and perhaps V2) significant of anything?
Brown is not totally familiar with that term, could you please clarify?
Thanks mate
Dutch-EMT
BScN
- 97
- 1
- 8
Sinusrhytm, 100/min. No atrial hypertrophy i think.
P-Q is at the limit, but a AV-Block??? Can be!!
LBBB (deep S in V1 and R-R' (M-shape) in V5).
Can't conclude a MI with a BBB!!!
P-Q is at the limit, but a AV-Block??? Can be!!
LBBB (deep S in V1 and R-R' (M-shape) in V5).
Can't conclude a MI with a BBB!!!
TomB
Forum Captain
- 393
- 82
- 28
That's a myth.
You can conclude acute STEMI in the presence of LBBB by using Sgarbossa's criteria including the modified form suggested by Stephen Smith, M.D. of Dr. Smith's ECG Blog (serial ECGs are also helpful).
http://ems12lead.com/2010/12/29/excessive-discordance-as-a-marker-of-acute-stemi-in-lbbb/
AMI is different from acute STEMI in that it includes NSTEMI which could have a nondiagnostic ECG but a rise and fall of cardiac biomarkers.
For our purposes what is most important is to identify patients with an acute thrombotic lesion in an epicardial coronary artery.
You can conclude acute STEMI in the presence of LBBB by using Sgarbossa's criteria including the modified form suggested by Stephen Smith, M.D. of Dr. Smith's ECG Blog (serial ECGs are also helpful).
http://ems12lead.com/2010/12/29/excessive-discordance-as-a-marker-of-acute-stemi-in-lbbb/
AMI is different from acute STEMI in that it includes NSTEMI which could have a nondiagnostic ECG but a rise and fall of cardiac biomarkers.
For our purposes what is most important is to identify patients with an acute thrombotic lesion in an epicardial coronary artery.