I'm trying to understand reciprocal changes leading to the interpretation of a Posterior wall MI.
Is it basically if you have ST elevation in the inferior leads + reciprocal depression in the Anterioseptal leads, that automatically means it's a posterior wall MI? This is a concept we are just being introduced to in school, so I apologize if I'm not using proper terminology.
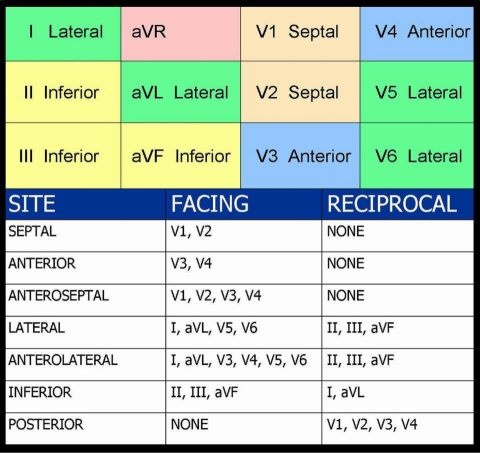
Here's the guide we were given to review:

Is it basically if you have ST elevation in the inferior leads + reciprocal depression in the Anterioseptal leads, that automatically means it's a posterior wall MI? This is a concept we are just being introduced to in school, so I apologize if I'm not using proper terminology.
Here's the guide we were given to review: