captaindepth
Forum Lieutenant
- 151
- 60
- 28
Snapped this really interesting EKG the other day. The pt was an extremely poor historian from an independent living facility and staff was not much help either.
All vital signs WNL, pt denies any C/P, SOB, or dizziness and only states he has had increased weakness over the past 48 hours with intermittent N/V. Only medical hx was diabetes which is controlled via oral medications, no drug or alcohol use reported reported or suspected. The pt adamantly wants to refuse transport.
What do you think?
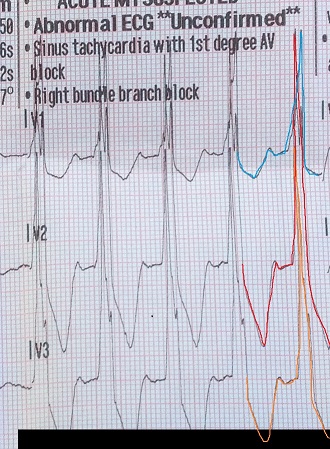
 ). I usually see this in lead V5 and V6 in some LBBB that have a biphasic T-wave and a tiny terminal S-wave. Computer probably tripping about there being an MI due to the excessive ST changes. I don't feel like the computer usually takes into consideration the amplitude of the QRS complexes so it commonly screams MIs on things like LBBB and LVH.
). I usually see this in lead V5 and V6 in some LBBB that have a biphasic T-wave and a tiny terminal S-wave. Computer probably tripping about there being an MI due to the excessive ST changes. I don't feel like the computer usually takes into consideration the amplitude of the QRS complexes so it commonly screams MIs on things like LBBB and LVH.