Can some of you seasoned healthcare professionals maybe clue me into what I'm reading here. Here is a direct lesson from class that I am just not clear on. If you have pictures that could help me understand this concept,i'd really appreciate it. thanks so much!
The mean vector is the average of all the electrical forces of the ventricles. This is the mean electrical axis or mean QRS axis of the heart. By superimposing the hexaxial reference figure over the heart, the normal axis can be seen to be between 0 and 90o. Many cardiologists extend the range + 30o of this value (-30o to 120o).
There are several methods of determining the mean QRS axis of the patient's heart by viewing the tracings from the six limb leads of the ECG. The following are two methods:
Method 1: Locate the largest QRS complex on the tracing, either negative or positive deflection.
(where i get lost).........
If the deflection is negative, then the cardiac vector is going opposite to the lead axis of the largest deflection and so the value for the cardiac vector will be the number of degrees opposite the lead axis value.
If the deflection is positive, then the cardiac vector is going the same direction as the lead axis of the largest deflection and so the value for the cardiac vector will be the same number of the degrees as the lead axis value.
Method 2: Locate the most equiphasic lead. An equiphasic QRS is in the ECG lead that is at right.angles to the QRS axis. Locate the lead that is at right angles to the most equiphasic lead. Then look to see if the deflection of the lead at right angles to the equiphasic lead is positive or negative.
If the deflection is negative, then the cardiac vector is going opposite to the lead axis of the largest deflection and so the value for the cardiac vector will be the number of degrees opposite the lead axis value.
If the deflection is positive, then the cardiac vector is going the same direction as the lead axis of the largest deflection and so the value for the cardiac vector will be the same number of the degrees as the lead axisvalue.
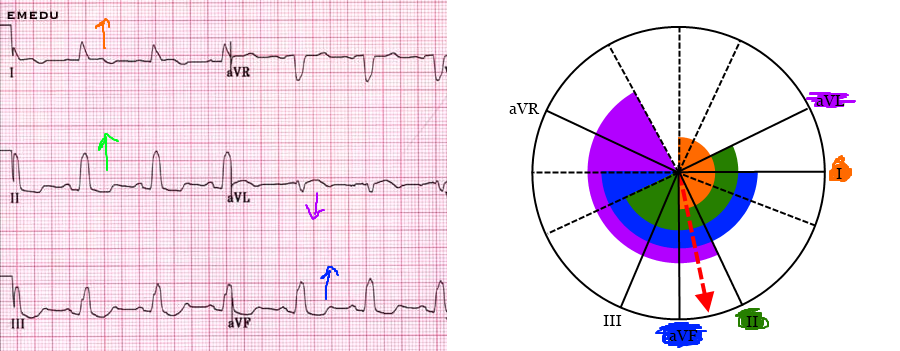
This schematic of the QRS complexes of the six limb leads will be used to the cardiac vector using both methods and the hexaxial reference figure.
Method 1: The largest R wave deflection is seen in Lead II. Since the deflection is positive this means that the lead axis and the cardiac vector are traveling in the same direction. Looking at the hexaxial reference figure, the axis for Lead II is 60o, so the cardiac vector for the patient is the same value of 60o.
Method 2: The most equiphasic lead is AVL. This means that this lead is perpendicular or at a right angle to the lead which will be the cardiac vector. Looking at the hexaxial reference figure, AVL is at a 90o or right angle to Lead II which will be the cardiac vector. Now we look back at the tracing to see if Lead II is positive or negative. It is positive, so the lead axis and cardiac vector are traveling the same direction. Looking at the hexaxial reference figure, the axis for Lead II is 60o and so the cardiac vector for the patient will also be 60o.
Often the cardiac vector will be the same for each method, but once again variations will occur with patients. In the lab we will be using the above information to calculate the cardiac vector with the traces we obtain. The cardiac vector gives us information on the tilt of the heart in a patient’s chest, which will vary between patients.
The mean vector is the average of all the electrical forces of the ventricles. This is the mean electrical axis or mean QRS axis of the heart. By superimposing the hexaxial reference figure over the heart, the normal axis can be seen to be between 0 and 90o. Many cardiologists extend the range + 30o of this value (-30o to 120o).
There are several methods of determining the mean QRS axis of the patient's heart by viewing the tracings from the six limb leads of the ECG. The following are two methods:
Method 1: Locate the largest QRS complex on the tracing, either negative or positive deflection.
(where i get lost).........
If the deflection is negative, then the cardiac vector is going opposite to the lead axis of the largest deflection and so the value for the cardiac vector will be the number of degrees opposite the lead axis value.
If the deflection is positive, then the cardiac vector is going the same direction as the lead axis of the largest deflection and so the value for the cardiac vector will be the same number of the degrees as the lead axis value.
Method 2: Locate the most equiphasic lead. An equiphasic QRS is in the ECG lead that is at right.angles to the QRS axis. Locate the lead that is at right angles to the most equiphasic lead. Then look to see if the deflection of the lead at right angles to the equiphasic lead is positive or negative.
If the deflection is negative, then the cardiac vector is going opposite to the lead axis of the largest deflection and so the value for the cardiac vector will be the number of degrees opposite the lead axis value.
If the deflection is positive, then the cardiac vector is going the same direction as the lead axis of the largest deflection and so the value for the cardiac vector will be the same number of the degrees as the lead axisvalue.
This schematic of the QRS complexes of the six limb leads will be used to the cardiac vector using both methods and the hexaxial reference figure.
Method 1: The largest R wave deflection is seen in Lead II. Since the deflection is positive this means that the lead axis and the cardiac vector are traveling in the same direction. Looking at the hexaxial reference figure, the axis for Lead II is 60o, so the cardiac vector for the patient is the same value of 60o.
Method 2: The most equiphasic lead is AVL. This means that this lead is perpendicular or at a right angle to the lead which will be the cardiac vector. Looking at the hexaxial reference figure, AVL is at a 90o or right angle to Lead II which will be the cardiac vector. Now we look back at the tracing to see if Lead II is positive or negative. It is positive, so the lead axis and cardiac vector are traveling the same direction. Looking at the hexaxial reference figure, the axis for Lead II is 60o and so the cardiac vector for the patient will also be 60o.
Often the cardiac vector will be the same for each method, but once again variations will occur with patients. In the lab we will be using the above information to calculate the cardiac vector with the traces we obtain. The cardiac vector gives us information on the tilt of the heart in a patient’s chest, which will vary between patients.
")