NPO
Forum Deputy Chief
- 1,831
- 897
- 113
Where do you personally draw the line? And if you're going with electrical therapy, do you premedicate?
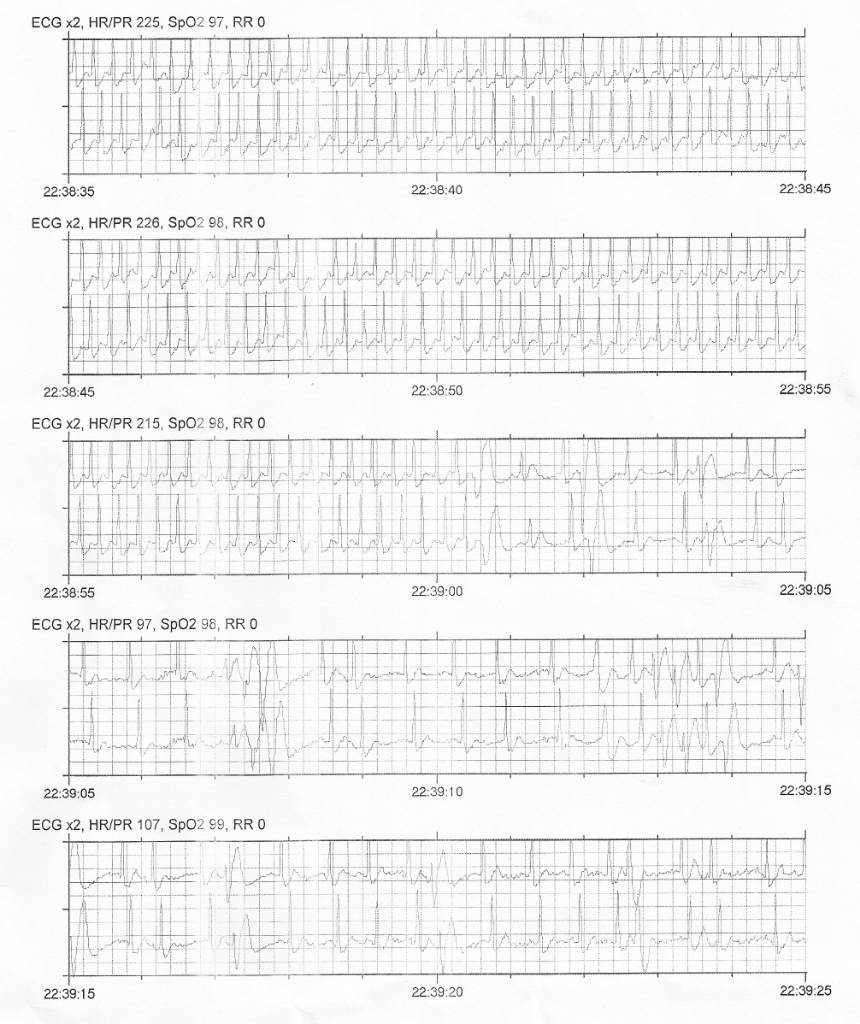
I had my first SVT, and by all means, I could have shocked him, and no one would have batted an eye. I even had my narcotics out and open. But I decided to give 6mg of Adenosine a try, just to say I did it; I didn't expect it to work, but it did.
The man called 911 complaining of chest pain, but he appeared in no significant distress. He was alert, oriented, and ambulatory on scene. His rate was 220, with a BP of about 85/50. I know this meets every indicator to move straight to electrical therapy, but given how non-symptomatic he appeared, I couldn't move past at least trying Adenosine first.
Sent from my Pixel XL using Tapatalk
I had my first SVT, and by all means, I could have shocked him, and no one would have batted an eye. I even had my narcotics out and open. But I decided to give 6mg of Adenosine a try, just to say I did it; I didn't expect it to work, but it did.
The man called 911 complaining of chest pain, but he appeared in no significant distress. He was alert, oriented, and ambulatory on scene. His rate was 220, with a BP of about 85/50. I know this meets every indicator to move straight to electrical therapy, but given how non-symptomatic he appeared, I couldn't move past at least trying Adenosine first.
Sent from my Pixel XL using Tapatalk