Angel Barrientos
Forum Ride Along
- 3
- 0
- 1
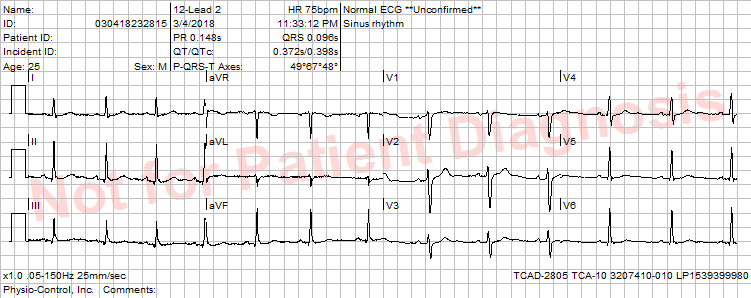
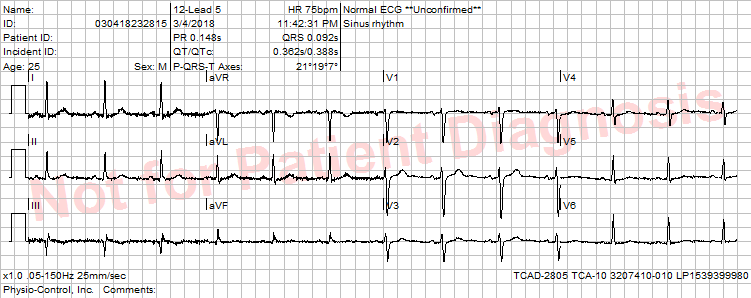
What are the Pros and Cons of placing the RA and LA leads on the forearm vs. placing the same leads right on the deltoids? As an EMT, I was always told to place the leads on the forearms or wrist by the Firefighter paramedics, but some of my clinical instructors have said that is wrong or that it provides a less accurate reading. Is this true? What is the best 12- lead placement? Links to research articles or resources will be much appreciated. Thank you for your time!